Download
1 / 82
820 likes | 918 Vues
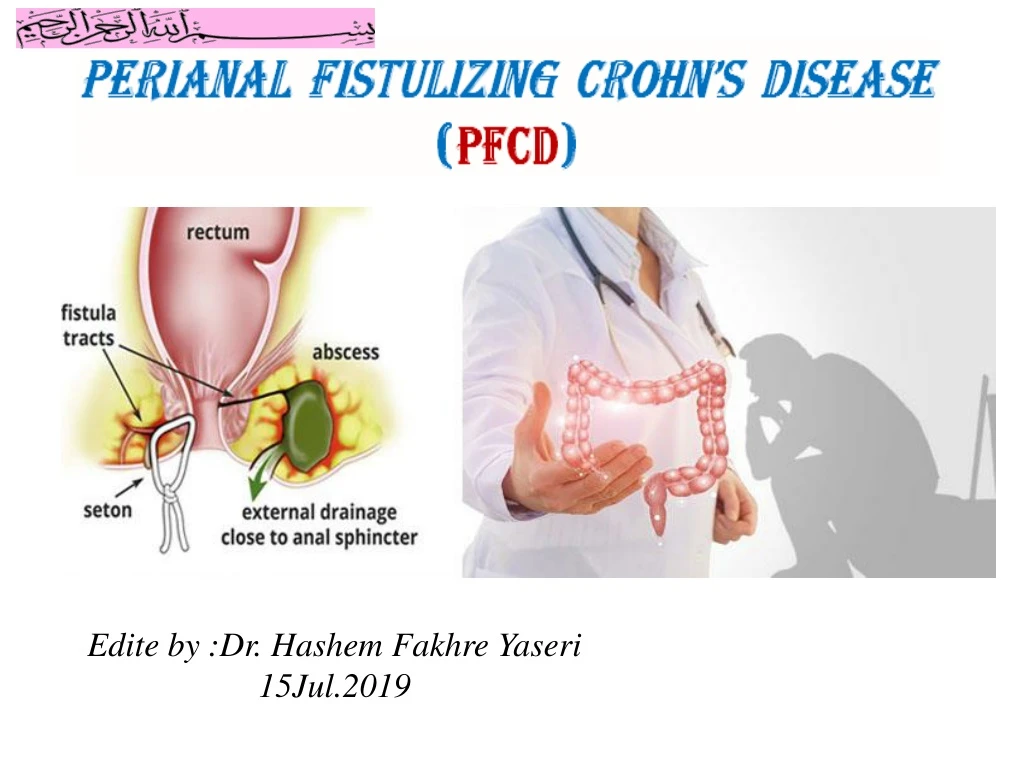
Edite by :Dr. Hashem Fakhre Yaseri 15Jul.2019. Perianal Fistulas in Patients With Crohn’s Disease, Part 1 : Current Medical ManagementStephanie L. Gold, Shirley Cohen- Mekelburg ,Yecheskel Schneider and Adam Steinlauf . Gastroenterology & Hepatology August 2018 - Volume 14, Issue 8.

E N D
Edite by :Dr. HashemFakhreYaseri 15Jul.2019
Perianal Fistulas in Patients With Crohn’s Disease, Part 1: Current Medical ManagementStephanieL. Gold, Shirley Cohen-Mekelburg,Yecheskel Schneider and Adam Steinlauf. Gastroenterology& HepatologyAugust 2018 - Volume 14, Issue 8 Perianal Fistulas in Patients With Crohn’s Disease, Part 2: Surgical, Endoscopic, and Future Therapies.Stephanie L. Gold,Shirley Cohen-Mekelburg,Yecheskel Schneider and Adam Steinlauf.Gastroenterology & HepatologyVolume 14, Issue 9 September 2018
Anatomy of anorectal Internal anal sphincter Levator Ani EXternal anal sphincter
Anal Abscess • Infected cavity filled with pus found near the anus or rectum. • 90% abscesses are the result of an acute infection in the internal glands of the anus. • Bacteria, fecal material or foreign matter can clog an Anal gland and tunnel into the tissue around the anus or rectum, where it may then collect in a cavity called an Abscess
Classification of anal Abscesses • Anal abscesses are classified by their location in relation to the structures comprising and surrounding the anus and rectum: • Perianal(Most frequent ) • Ischioanal • Inter-sphincteric • Supra-levator (Least frequent )
Classification of anal Abscesses Horse-shoe Abscesses • If any of these particular types of Abscess spreads partially andcircumferentially around the Anus or the rectum, it is termed a Horse-shoe Abscesses. HorseshoeAbscesses
Definition of Various Types of Perianal Lesions in Patients With Crohn’s Disease AGA Technical Review on Perianal Crohn’s Disease.Gastroentrology.2003;125:1508–30
Fistulas • Two different intestinal segments • Two different organs • An organ to the outside of the body • Abnormal communication between two epithelial-lined surfaces. • Fistula is a hollow tube of tissue connecting : • Examples of fistulas include:
Anal fistula ( Fistula-in-ano ) Cryptoglandular hypothesis Definition • An epithelialized track that can form and connects the Abscess in the anus or rectum(Anorectum)with the peri-rectal skin • Anal fistulas are sometimes also referred to as “Fistula-in-ano “
Cryptoglandular hypothesis • Perianal Abscess that contains gut flora commonly leads to the development of anal fistula • Some times bacteria are infrequently found in chronic fistulas • Recent work has shown an increased expression of pro-inflammatory cytokines and epithelial to mesenchymal cell transition in both Cryptoglandular and Crohn’sPerianal fistulas. Sugrue et .Techniques in Coloproctology June .2017;21;(6);425–32
Etiology Fistula-in-ano(Anal Fistula) • Infected Anal Crypt gland • Crohn disease (CD) • Tuberclusion • Rectal foreign bodies • Lymphogranulomavenereum (Chlamydia trachomatis) • Radiation proctitis (Pelvic radiation) • Actinomycosis (Immunocompromised patients) • Obstetric injury (Prolonged labor)
Differential Diagnosis of Fistula-in-ano • Infection • Cryptoglandular • Tuberclusion • Actinomycosis • Lymphogranulomavenereum • Pelvic inflamatory disease • Appendicitis • Specific • Nonspecific(90%) • Trauma • Foreign body • Obstetric • Hemorrhoidectomy • IBD • Cancer • Extra-anal sources • Presacral cyst • Bartholins cyst • Pilonidal disease • Hidradenitissuppurativa • Adenocarcinoma of the rectum • Squamous cell carcinoma of the anus • Lymphoma
Epidemiology PFCD • Perianal fistulizing Crohn’s disease (PFCD) has a serious impact on quality of life (QOL) and mental health . • Despite advancements in the Medical and Surgical treatment of CD over the past decade, Perianal fistulas still present a significant challenge to physicians. • Incidenceof an Anal fistula developing from an Anal abscess ranges from 26% to 38 % • Mean age for presentation of Anal abscess and Fistula disease is 40 years • Perianal fistulas can be the Initial manifestation of CD in 10% of the patients • Perianal fistulas affect roughly 5% to 40% of patients with CD
Epidemiology PFCD • Incidence PFCDincreases with more distal disease (ie, colonic and rectal involvement) than in those with isolated ileal disease as well as with increased disease duration and severity • Adult males are twice as likely to develop an Abscess and/or Fistula compared with women • A population-based study found that the incidence of Perianal fistula in patients with Crohn’s disease (CD) is 21–23% and that the Cumulative incidences of the condition at 1, 5, 10 and 20 years are 12%, 15%, 21% and 26%, respectively • Large prospective and retrospective studies have shown that two-thirds(2/3) of patients with PFCD experience Relapses XiaohanYan et al .Gastroenterology Report.7(1);2019;50–6
Epidemiology PFCD • Successful therapeutic management of Perianal fistulas would ideally include Complete fistula closure. • However, given the complexity of these lesions, many physicians have shifted their therapeutic Goal from Complete closure to Reductions in pain and Purulent drainage and an Improvement in quality of life(QOL) • Although various Medicationsand Endoscopicand Surgical techniques exist, there is no Gold-standard treatment strategy for patients with perianal fistulas. • Successful management requires a Multidisciplinary approach with a gastroenterologist and a colorectal surgeon.
Classification of Perianal fistula(Fistula-in-ano) • Several Perianal fistula classification systems have been described in the literature,themost common of which is the Parks classification (UK in 1976 have been described, before MRI or endoanal ultrasound was available) • Fistulas are classified by their relationship to parts of the anal sphincter
Classification of Perianal fistula(Fistula-in-ano) • Parks classification categorizes Perianal fistulas based on their relationship to the External and Internal Anal sphincters Park’s classification A- Superficial B- Inter- sphincteric C- Trans- sphincteric, D- Supra- sphincteric E- Extra-sphincteric ZIECH M.CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:1037–45
Classification of Perianal fistula(Fistula-in-ano) • Given the complexity of this classification, the American Gastroenterological Association (AGA) Technical Review Panel proposed a revised classification that defines perianal fistulas as either (Bell classification): • simple • complex • In comparison to the traditional Parks classification system, the AGA’s breakdown of fistulas into either simple or complex has proven to be much easier and more meaningful in the clinical setting, as a simple fistula is significantly easier to manage and poses little threat to fecal continence
2-Revised classification of (AGA) ( Bell classification ) • A simple fistula is one that is confined to the anal canal (either Superficial, Low Inter-sphincteric,Low Trans-sphincteric) or has a single opening in the skin, and does not have an associated Abscess • Simple: without any extention A,B,C
2-Revised classification of (AGA) ( Bell classification ) • Complex: without extention • A complex perianal fistula passes through or above a significant amount of muscle (either HighInters-phincteric, High Trans-sphincteric, Extra-sphincteric, or Supra-sphincteric) and is associated with multiple openings in the skin, a Perianal Abscess, or an Anorectal stricture
3- Classification of perianal fistula • Classification of Perianal fistula • Low level fistulas • Low level Fistulas or Low trans-sphincteric Fistulas involve the lower 3rd of the External anal sphincter mechanism • Tend to be either Idiopathic or associated with Anal gland infection • Generally treated by Fistulotomywith a high success rate for cure Anal gland
3- Classification of perianal fistula • Classification of Perianal fistula • High level fistulas • High level fistulas or High Trans-sphincteric fistulas involving the upper two thirds(2/3) of the external sphincter • Internal opening above the Levatorani • Remain a surgical challenge becauseFecal Incontinence(FI)
4-Goodsall's law • Classification of Perianal fistula Goodsall's law. • Fistulas with an Anterior external opening drain directly into anterior half of the anus at the dentate lineis Direct type • Fistulas with a Posterior external opening in relation to the posterior half of the anus ,has a curved track may be of Horse-shoe type, opens in the midline posteriorly and may present with multiple external opening all connected to a single internal opening. • Goodsall'slaw indicates that
Classification of Perianal fistula 5-Classification Perianal fistula • Single External opening • Multiple External opening Which are often seen in • Tuberculosis • Ulcerative colitis • Crohns disease • Hidradenitissuppurative • Actinomycosis
James University Hospital Classification - MRI-based grading system for perianal fistulas ZIECH M.CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:1037–45
Perianal Fistulas in Patients With Crohn’s Disease, Part 1: Current Medical ManagementStephanieL. Gold, Shirley Cohen-Mekelburg,Yecheskel Schneider and Adam Steinlauf. Gastroenterology& HepatologyAugust 2018 - Volume 14, Issue 8 Perianal Fistulas in Patients With Crohn’s Disease, Part 2: Surgical, Endoscopic, and Future Therapies.Stephanie L. Gold,Shirley Cohen-Mekelburg,Yecheskel Schneider and Adam Steinlauf.Gastroenterology & HepatologyVolume 14, Issue 9 September 2018
Perianal Fistulas in Patients With Crohn’s Disease, Part 1: Current Medical ManagementStephanie L. Gold, Shirley Cohen-Mekelburg,Yecheskel Schneider and Adam Steinlauf Gastroenterology & Hepatology August 2018 - Volume 14, Issue 8;470-80
Management Perianal Fistulizing Crohn’s disease (PFCD) Surgical therapy Medical therapy Favour • Medical • Surgical
Management Perianal Fistulizing Crohn’s disease (PFCD) • Surgical
Management Perianal Fistulizing Crohn’s disease (PFCD) • 1 - Medical • Systemic • Local • Antibiotics (Metronidazole,Ciprofloxacin ) • Immunomodulators[Thiopurines,Methotrexate,Tacrolimus,CyclosporineA, Thalidomide,MycophenolateMofetil] • Biologic Agents [Infliximab,Adalimumab,CertolizumabPegol,Vedolizumab,Ustekinumab] • Hyperbaric Oxygen Therapy (HOT) • Adsorbent Carbon
Antibiotics Medical management • Antibiotics such as Metronidazoleand Ciprofloxacin have been used as first-line therapy for patients with Fistulizing CD, although data supporting their efficacy are limited to small studies • In one of the initial studies evaluating Metronidazoleuse, 56% of patients had Fistula closure after 6-8 weeks of therapy. • Suggested that Metronidazole is effective at inducing Fistula closure, Recurrence rates • Brandt et al, studied Metronidazoleuse in patients with Perianal fistulasand found that only 28% of patients who had Fistula healing were able to successfully discontinue therapy without recurrence
Antibiotics Cont.1-Medical management • Long-term use of Antibiotics is associated with significant morbidity • No clinical Guidelineson Antibiotic selection exist, but Ciprofloxacin has been shown to have higher rates of clinical improvement and Complete fistula closure when compared to Metronidazole, although the difference did not reach significance • Use of TopicalAntibiotic ointments or creams for patients with Perianal CD has been investigated • A randomized trial assessing the use of Metronidazole topical ointmentreported an improvement in painand drainagefrom the Fistula tract
Antibiotics Cont.Medical management • Although the use of antibiotics as long-term monotherapyfor Perianal CD is not ideal, studies have evaluated the efficacy of Metronidazole or Ciprofloxacin as adjuvant therapy with Immunomodulators or biologic agents • In a prospective, open-label study looking at Fistula closure, combination therapy of Metronidazole and/or Ciprofloxacin with Azathioprine(AZA) was significantly more effective at achieving a clinical response (48%) when compared to Metronidazole and/or Ciprofloxacin alone (15%).
Antibiotics Cont.Medical management • A double-blind, placebo-controlled study demonstrated that patients treated with Infliximab and Ciprofloxacin tended to have a better clinical response than patients treated with infliximab and a placebo (odds ratio[OR],2.37; P=.07). • Dewint et al. evaluated the use of Ciprofloxacin in combination with Adalimumabfor patients with CD and found a Clinical response in 71% of patients treated with Adalimumab and Ciprofloxacin compared with 47% of patients treated with Adalimumab and Placebo (P=.047)
Table 1. Studies on Antibiotic Therapies for Perianal Fistula Closure NNT, number needed to treat; PDCAI, Pediatric Crohn’s Disease Activity Index; RCT, randomized, controlled trial. aTheNNT is 1/absolute risk reduction
Antibiotics Cont.Medical management These studies suggest that although Antibioticsare not useful for long-term monotherapy, they can be effective as a bridgeor as adjuvant therapy when combined with Immunomodulators or Biologic agents.
Immunomodulators Medical management 1-Thiopurines • AZAand 6-Mercaptopurine(6-MP) are commonly used for the treatment of Perianal fistulas in patients with CD. • In the only prospective, randomized trial evaluating the efficacy of Thiopurinesin patients with fistulizingCD, 6-MP was found to be effective at inducing complete fistula healing • 43% (9/21) of patients treated with 6-MP had complete fistula closure compared to 6% (1/17) of patients receiving a placebo
Immunomodulators Cont.Medical management 1-Thiopurines • A meta-analysis by Pearson et al, found that 54% (22/41) of patients with perianal CD who were treated with 6-MP or AZA had clinical improvement compared with 21% (6/29) of patients who received a placebo, with a pooled OR of 4.44 favoring fistula healing.
Immunomodulators Cont.Medical management 1-Thiopurines • Korelitzet al,demonstratedthat 38% (13/34) of patients treated with 6-MP had Complete fistula closure after 6 months of therapy, and an additional 26% (9/34) of patients had Clinical improvement • In a Pediatric study, Jeshion et al concluded that 67% of patients treated with AZA or 6-MP had improvement in fistula drainage, 73% had improvement in perianal tenderness, and 40% had fistula closure
Immunomodulators Cont.Medical management 2-Methotrexate(MTX) • Methotrexateis commonly used in patients with CD, the data are limited regarding its effect on perianal disease. • Mahadevanet al, published one of the only studies to date evaluating the efficacy of intramuscular Methotrexate on fistula closure • In this case series, 25% (4/16) of patients receiving Methotrexate had fistula closure, and an additional 31% (5/16) of patients had fistula improvement • Interestingly, when switching to Oral Methotrexate or lowering the dose of intramuscular methotrexate, the majority of patients had Fistula recurrence.
Immunomodulators Medical management 3-Tacrolimus • Tacrolimusis commonly used in patients who have undergone Solid organ transplantation;however, some studies have suggested that the drug can be beneficial in patients with CD • A randomized, controlled trial investigating the efficacy of oral Tacrolimusin patients with Fistulizing CD found that 43% of patients treated with tacrolimus had fistula improvement compared with 8% of patients in the placebo group
Immunomodulators Cont.Medical management 3-Tacrolimus • Gonzalez-Lama et al, studied the use of Tacrolimus in 10 patients with Fistulizing CD, and documented complete closure in 40% of patients and a partial clinical response in 50% of patients treated for 6 to 24 months. • Research on topical Tacrolimusin patients with Perianal disease suggests possible efficacy in improving symptoms but not in inducing complete closure
Immunomodulators Medical management 4-Cyclosporine A(CSA) • Multiple randomized, placebo-controlled trials have evaluated the efficacy of Cyclosporine A (CSA) in patients with CD, none have specifically focused on fistula closure • In a case series of 16 patients treated with CSA, Presentet al, reported Complete closure in 44% (7/16) of patients and Moderate improvement in an additional 44% (7/16) of patients treated with Intravenous CSA over an average of 7.4 days 17. Lichtenstein GR. Treatment of fistulizing Crohn’s disease. Gastroenterology. 2000;119(4):1132-1147.
Immunomodulators Cont.Medical management 4- Cyclosporine A(CSA) • Interestingly, of the 10 patients who had previously failed6-MP and/or AZA in this study, 9 patients (90%) had improvement in the Fistulawhen treated with CSA. • In another study evaluating in patients treated with intravenous CSA, 78% of patients showed a Partial clinical response; however, 71% of those patients who were ultimately converted to Oral CSA ,had relapse of their disease • Therefore,CSA is likely best used as an intravenous rescue bridge to a more long-term Immunomodulator or Biologic therapy.
Immunomodulators Medical management 5 - Thalidomide • In patients with severely Refractory disease, the use of Thalidomidehas been proposed. • To date,2 small studies in patients with FistulizingCD treated with Thalidomide are available. • Plamondonet al,evaluated the use of Thalidomide for patients with Refractory CD and included 4 patients with Perianal fistulas, all of whom had documented Complete closure. • However, nearly 50% of the entire cohort terminated the use of Thalidomidedue to severe side effects, including neuropathy and leukopenia.
Immunomodulators Cont.1-Medical management 5 - Thalidomide • Ehrenpreis et al, performed an open-label trial looking at the use of Thalidomidein patients with Refractory CD. • Inthis study, 46% (6/13) of patients with a Perianal fistula had clinical improvement in the fistula after 12 weeks of therapy • Lenalidomide (Revlimid), an analogue of Thalidomide, has the potential to be effective with significantly less toxicity, although its use in CD has not been studied
Immunomodulators Medical management 6-Mycophenolate Mofetil(Celcept) • Mycophenolatemofetil,animmunomodulatorless commonly used to treat patients with CD, has been shown to be effective in patients with Fistulizing disease. • In a study evaluating 4 patients with treatment Refractory Perianal disease, 75% (3/4) had Complete fistula closure for the first time in their clinical course.
Table 2. Studies on Immunomodulator Therapies for Perianal Fistula Closure 6-MP, 6-mercaptopurine; AZA, azathioprine; NNT, number needed to treat; RCT, randomized, controlled trial. aTheNNT is 1/absolute risk reduction.
















