Download
1 / 21
210 likes | 375 Vues
Case Study 3: Heart and Peripheral Vascular. University of North Carolina Wilmington NSG 250 Christy Pope, Sarah Orial , Stephanie Carpico , Jennifer Feagan. Background Information.

E N D
Case Study 3: Heart and Peripheral Vascular University of North Carolina Wilmington NSG 250 Christy Pope, Sarah Orial, Stephanie Carpico, Jennifer Feagan
Background Information • Mr. Madison is a 69 year old African American school teacher who is brought to the E.R. for evaluation of chest pain. While shoveling snow Mr. Madison suddenly felt short of breath and dizzy. He described his chest pain to be “crushing and heavy” and radiating to his left arm. Mr. Madison’s chest pain subsided to a 2/10 pain after taking two Nitroglycerin tabs and resting on the couch. His wife proceeded to call the ambulance.
Background Information Cont. • While Mr. Madison is having his EKG, his wife pulls the nurse aside to tell her that he has a medical history of hypertension, high cholesterol and diabetes. • However, he has not been taking his medication for the last year, since he quit smoking. • Mrs. Madison also says her husband is about 50 pounds overweight because he eats whatever he wants and does not get much exercise. • Mr. Madison states he is very upset, because his Dad died of a heart attack.
Subjective Data • Chest pain “crushing, heavy and radiating down arm” • Chest pain now a 2/10 after two Nitro • Shortness of breath • Dizziness • Nausea • Family history of heart attack “father died at 52” • History of hypertension, high cholesterol and diabetes • Former smoker “quit last summer” • Medication non-compliance “hasn’t taken in a year” • No dietary restrictions “uses salt shaker freely”
Objective Data • Heart Rate is 118 • Blood Pressure is 172/98 mm Hg • Heart Rhythm is regular, S1 and S2 heard with murmurs of extra sounds • Diaphoretic skin • Appears anxious • Palpable apical impulse at the 5th intercostal space • No heaves, pulsations of lifts are evident over precordium
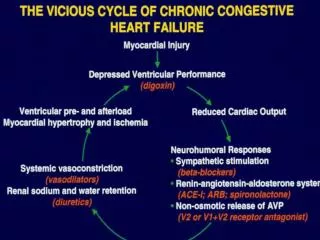
Myocardial Infarction • Based on the collected data it appears Mr. Madison may be having a myocardial infarction better known as a heart attack. • Onset: Started this morning, lasted about 10-20 minuets • Location: Chest and radiating down his left arm • Character: Crushing and heavy • Pain brought on by: Exertion while shoveling the driveway • Associated symptoms: diaphoretic, nausea, shortness of breath and dizziness • Relieved by: rest and 2 nitro tablets
Interventions: MONA • Morphine- typically 2-4 mg IV • Oxygen – 4 liter per min via nasal cannula • Nitro – 1 sublingual tab every 5 min, up to 3 doses • Aspirin – 325 mg by mouth
Diagnostics: EKG • Once Mr. Madison’s EKG is complete, the doctor will review it to look for EKG changes • He will look for elevation of the ST segment, which indicates a STEMI (ST Elevated Myocardial Infarction). • A STEMI, is a life threating emergency requiring immediate intervention.
Diagnostics: Blood Work • Mr. Madison will need a set of cardiac enzymes typically drawn every 6 hours, times 3 sets. • Cardiac enzymes consist of Troponin, CK and CKMB. • An elevated Troponin level is most indicative of cardiac muscle damage and heart attack. • Other blood work such as cholesterol and glucose levels should also be drawn because we know they play such a vital role on the cardiovascular system.
Diagnostics: Stress Test • Mr. Madison may be asked to participate in a stress test. • Mr. Madison can only have a stress test if his cardiac enzymes were negative. • There are two types: traditional and nuclear. • During the stress test Mr. Madison will walk on a treadmill while having his EKG and blood pressure monitored. • The nuclear stress test is most beneficial because a dye is injected into the bloodstream and pictures are taken of the heart that can show if there are any blockages. • Stress test is only for diagnostic purposes, no intervention can be done during a stress test.
Intervention: Catheterization • If blockages are seen during Mr. Madison’s stress test he will need to have a cardiac catheterization. • A cardiac catheterization is a invasive procedure done under moderate sedation, a consent must be obtained. • During a cardiac cath a thin flexible tube is inserted into the femoral artery and dye is injected into the blood stream. • Pictures are then taken of the heart and blockages may be seen. If a blockage is seen a angioplasty or stent my be done to reopen the narrowed artery.
Modifiable Cardiac Risk Factors • Weight • Diet • Smoking • Exercise • Stress • Non-compliance
Non Modifiable Risk Factors • Gender - Male • Genetics – Family history • Age – Greater then 50 • Race – African American
Cultural Considerations • Heart disease is the number one killer for all Americans, but the chance is higher among African American’s. • High blood pressure, obesity and diabetes are the most common conditions that increase the risk of heart disease. Mr. Madison has all of these. • The prevalence of high blood pressure in African-Americans is the highest in the world. Research suggests African-Americans may carry a gene that makes them more salt sensitive, increasing the risk of high blood pressure. • African-Americans are disproportionately affected by obesity. Among non-Hispanic blacks age 20 and older, 63% of men and 77% of women are overweight or obese. • African-Americans are nearly twice as likely to have diabetes as non-Hispanic whites. In fact, about 15% of all African-Americans age 20 and older have the disease. • In 2009, African Americans were 30% more likely to die from heart disease, as compared to non-Hispanic white men.
Nursing Diagnosis • Acute Pain related to ischemic tissue, secondary to clogged arteries. • Decreased Cardiac Output related to changes in power factors, reduction of myocardial characteristics. • Activity Intolerance related to the imbalance between oxygen supply and demand, the ischemic / necrotic tissue • Ineffective Tissue Perfusion related to ischemic heart muscle damage, narrowing / blockage of coronary arteries. • Anxiety related to actual threats to biological integrity • Knowledge deficit related to sedentary lifestyle, poor diet and medication non compliance
Patient Education • For the first time, the American Heart Association has defined what it means to have ideal cardiovascular health, identifying seven health and behavior factors that impact health and quality of life. We know that even simple, small changes can make a big difference in living a better life. Known as “Life’s Simple 7,” these steps can help add years to your life: • don’t smoke • maintain a healthy weight • engage in regular physical activity • eat a healthy diet • manage blood pressure • take charge of cholesterol • keep blood sugar, or glucose, at healthy levels
Diet Education • The American Heart Association’s Heart Healthy Diet Recommendations are based on a 2,000 calorie diet and include: • Limit saturated and trans fat and cholesterol by choosing lean meats, selecting fat-free (skim), 1 percent and low-fat dairy products and avoiding hydrogenated fats (margarine, shortening, cooking oils and the foods made from them). • Choose and prepare foods with little or no salt (sodium) to maintain a healthy blood pressure. Keep sodium intake to 1,500 mg per day or less. • Eat fish, especially oily fish like salmon or albacore tuna, twice a week to get omega-3 fatty acids. • Make your diet rich in fruits and vegetables. A typical adult should try for 9-10 servings (4.5 cups) of fruits and vegetables every day. • Limit or avoid alcohol
Exercise Education • After a heart attack most doctors recommend aerobic cardiovascular exercise. Aerobic exercise includes activities such as walking, jogging, cycling, and swimming. Mr. Madison’s doctor and the cardiac rehabilitation staff will determine the exact type and intensity of exercise he should do. Although his initial workouts will likely be at a low intensity level and later ones likely will be more intense, a typical workout may include the following: • about 10 minutes of warm-up (that is, stretching or light walking, jogging, or cycling) • 20 to 30 minutes of more intense cardiovascular exercise • 5 minutes of cool-down (with activities similar to the warm-up) • Doctors usually request that heart attack patients exercise at least three times a week
Medication Education • Mr. Madison will be going home with new prescription medications, it is very important that he be educated and provided with patient handouts about theses medications • Because Mr. Madison has a history of medication non compliance the importance of taking his medication daily needs to be reiterated. • One study showed that patients who do not take their medications after their first heart attack increase their chances of dying within a year by 80%
Best Place to Listen to Heart • The examiner places the stethoscope over 4 areas of the chest to listen to the valves of the heart to pick up a possibility of heart murmurs. To listen to the pulmonary valve the stethoscope is placed over the second intercostal space (the space between the 2nd and 3rd rib) on the left side of the patient’s sternum. The aortic valve is heard over the 2nd intercostal space on the right side of the patient’s sternum. The tricuspid valve is heard over the 5th intercostal space at the left side of the patient’s chest. The mitral valve is heard over the 5th intercostal space inline with the middle of the collar bone. • First heart sound (S1) can be heard loudest at the apex of the heart and second heart sound (S2) can be heard loudest at the base.
African Americans and Heart Disease . (2012, November 9). Retrieved from American Heart Association: http://www.heart.org/HEARTORG/Conditions/More/MyHeartandStrokeNews/African - Americans - and - Heart - Disease - Stroke_UCM_444863_Article.jsp Cardiac Auscultation . (2012). Retrieved from Heart Disease and Prevention: http://www.heart - disease - and - prevention.com/cardiac_auscultation.html Healthy Diet Goals . (2012). Retrieved from American Heart Association: http://www.heart.org/HEARTORG/GettingHealthy/NutritionCenter/H ealthyDietGoals/Healthy - Diet - Goals_UCM_310436_SubHomePage.jsp Heart Disease and African Americans . (2012, August 9). Retrieved from Office of Minority Health: http://minorityhealth.hhs.gov/templates/content.aspx?id=3018 Jarvis, C. (2012). Physical Examana tion and Health Assessment. St Louis: Elsevier Saunders. Johns Hopkins. (2007, April 20). Exercising Safely After a Heart Attack . Retrieved from Heart Health Special Report: http://www.johnshopkinshealthalerts.com/reports/heart_health/261 - 1.html Wascher, R. (2008, March 2). Medication Compliance & Risk of Death After Heart Attack. Retrieved from Health Report: http://doctorwascher.com/Archives/3 - 2 - 08 References