Download
1 / 20
210 likes | 1.2k Vues
CHAPTER 16 MUSCULAR DYSTROPHY AND JUVENILE RHEUMATOID ARTHRITIS (JRA). MUSCULAR DYSTROPHY ( ADD THE CASE STUDY FROM PAGE 237 HERE.).

E N D
CHAPTER 16MUSCULAR DYSTROPHYANDJUVENILE RHEUMATOID ARTHRITIS (JRA)
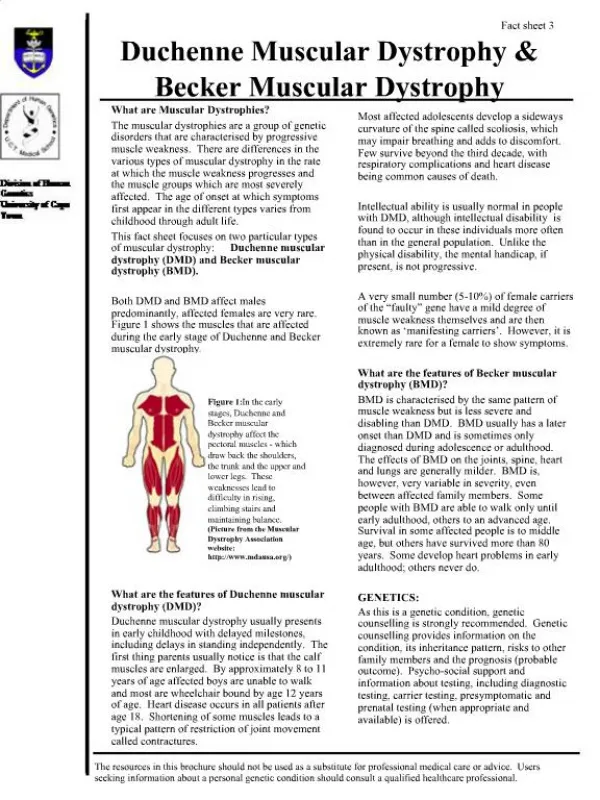
I. Definition – Skeletal neuromuscular disease is characterized by persistent deterioration of striated muscle tissue. Muscular Dystrophy is distinguished from other Neuromuscular diseases by four criteria: • 1. Primary myopathy • 2. Genetic base • 3. Progressive nature • 4. Degeneration of muscle fibers
The disease is a degeneration of muscle tissue in which muscle cells degenerate and the emergence of fat and fibrous tissue replaces muscle tissue. (Insert Figures 16.1 and 16.2 on page 239 here.) • Physical Characteristics as the disease progresses include: • Muscle weakness • Fatigue • Respiratory/heart complications
Types and Characteristics of Muscular Dystrophy (Insert Table 16.1 on page 238 here.) Progression through stages of functional ability include: 1. Low strength/endurance; normal ambulation with possible overwork weakness; slight deficiency in function. 2. Reduction in activity; tendency to fatigue easily; reduced strength/endurance; habitual activity, mild contractures and possible overwork weakness; ambulation with assistance.
3. Poor strength/endurance; overwork weakness; contractures; limited ambulation and decrease in physical activity and standing. 4. Ambulation significantly decreased; functional use of wheelchair; severe contractures and muscular weakness; pulmonary difficulties and cardiomyopathy.
Planning the Physical Activity Program: Individuals with muscular dystrophy commonly demonstrate low muscle endurance and fatigue quickly while walking and climbing stairs. Guidelines for Intervention: • Medical Approval - determine type and state; recommendations for intervention. • Assessment - Determine residual strength flexibility and functional capabilities. • Intensity - Avoid all out bouts of exercise. Use alternative resistance and water exercise to maintain functional ability.
Warm-up Cool-down: Critical component to prepare weakened muscle for work out. Facilitate strength, flexibility and maintaining function. • Implementing the Physical Activity Program - A. Concerns:Early recognition is essential for early intervention physical activity will help maintain muscular strength and functional ability. Recommendation for intervention should promote range of motion, maintain positive and alleviate contractures. Several concerns are evident in developing an excise program. They include:
Extent of muscle weakness • Progression of disease • Degree and intensity of the exercise • Individual needs B. Individualized Program Approach: The components of an exercise program should include strength, endurance and aerobic power that is essential for standing, walking and functional daily tasks. Goals of the program should include: • Provide short-term realistic goals • Focus on maintaining or reducing the rate of deterioration • Focus on submaximal exercises and reduce intensity to avoid fatigue • Prevent contractures and provide nutritional counseling • Provide activities in an enjoyable setting to facilitate compliance
C. Community Home Based Interventions (Insert Table 16.2 on page 244 here.)
JUVENILE RHEUMATOID ARTHRITIS (JRA)(Insert Case Study on page 245 here)
I. Definition - JRA • JRA is a general term for all types of arthritis and related conditions occurring (Arthritis Foundation 2009). The primary pathology of the chronic disease is inflammation of the connective tissues and is characterized by swelling and pain.
II. Symptoms and Types • Juvenile arthritis is characterized by major changes in the joints including inflammation, contractures and joint damage which affect mobility, strength, and endurance. • Nearly all children experience periods when symptoms reduce in severity or disappear but may go from symptom free to extreme pain and swelling • When children are symptom free they should be encouraged to participate in developmental activities
Psychological and social impacts are multidimensional as joint pain and stiffness becomes a distraction that effect concentration; medication schedules are also disruptive and have side effects – subtypes are distinguished by the number of joints involved within the first 6 months of onset: • Systemic arthritis – entire body is affected from high spiking fever to concomitant joint discomfort
Polyarticular arthritis – arthritis in five or more joints with major symptoms of pain in the knees, ankles, wrist, fingers, elbows and shoulders. Constant pain is prevalent • Pauciarticular arthritis - arthritis in four or fewer joints within the first 6 mo of onset; large joints of knee, ankle, elbow, and wrist are affected.
III. Planning the Physical Activity ProgramMedication • Nonsteroidal anti-inflammatory medication approved in children 12 and under although side effects are apparent • Glucocorticoid Drugs including cortisone and prednisone are used for pain and swelling. Side effects include high blood pressure, osteoporosis, weight gain and slower growth rate.
Exercise Considerations! • Physical activity and exercise are mainstays in treatment. The Arthritis Foundation recommends participation in physical activity which leads to the following benefits: • Maintains joint flexibility • Maintains muscle strength • Regains range of motion or strength in joint or muscle • Makes functional activities such as walking easier
Exercise Considerations! (contd.) • Improves general fitness and endurance • Improves self-esteem • Prevents deconditioning • Maintains bone density
IV. IMPLEMENTING THE PHYSICAL ACTIVITY PROGRAM Input is needed from the collaborative team and alleviating stress on their joints on joint protection. The Arthritis Foundation recommends 3 types of exercises: • Flexibility exercises for joint movement • Strengthening exercise including isometric and isotonic exercise to support and protect joints • Cardiovascular exercise to control weight and maintain functional ability Add Table 16.3 from page 249 here.
Learning Activity • Have your class identify several exercise programs developed by the Arthritis Foundation including the aquatics exercise program and walking with ease. Also contact the Center for Disease Control concerning the National Arthritis Action Plan.