Download
1 / 1
10 likes | 95 Vues
Management Challenge of Thrombophilia in Pregnancy-Case Report Dr. Gabriel Onyeka Ekekwe, Dr. Tempest Nicola, Mrs. Sandhya Rao St Helens & Knowsley Teaching Hospitals NHS Whiston Hospital, Warrington Road, Prescot, L35 5DR.

E N D
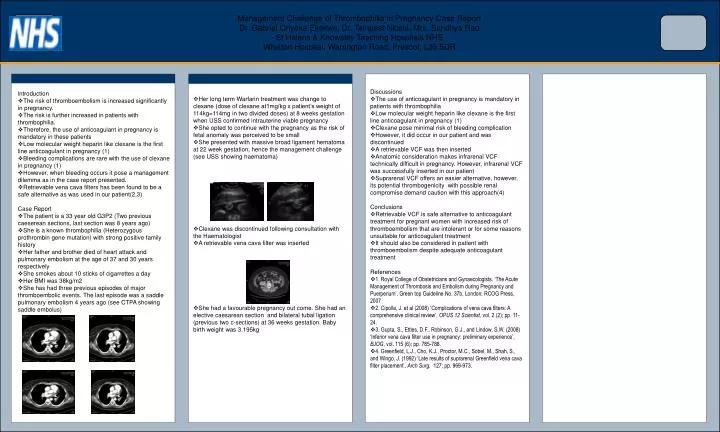
Management Challenge of Thrombophilia in Pregnancy-Case ReportDr. Gabriel Onyeka Ekekwe, Dr. Tempest Nicola, Mrs. Sandhya RaoSt Helens & Knowsley Teaching Hospitals NHSWhiston Hospital, Warrington Road, Prescot, L35 5DR • Her long term Warfarin treatment was change to clexane (dose of clexane at1mg/kg x patient’s weight of 114kg=114mg in two divided doses) at 8 weeks gestation when USS confirmed intrauterine viable pregnancy • She opted to continue with the pregnancy as the risk of fetal anomaly was perceived to be small • She presented with massive broad ligament hematoma at 22 week gestation, hence the management challenge (see USS showing haematoma) • Clexane was discontinued following consultation with the Haematologist • A retrievable vena cava filter was inserted • She had a favourable pregnancy out come. She had an elective caesarean section and bilateral tubal ligation (previous two c-sections) at 36 weeks gestation. Baby birth weight was 3.195kg • Discussions • The use of anticoagulant in pregnancy is mandatory in patients with thrombophilia • Low molecular weight heparin like clexane is the first line anticoagulant in pregnancy (1) • Clexane pose minimal risk of bleeding complication • However, it did occur in our patient and was discontinued • A retrievable VCF was then inserted • Anatomic consideration makes infrarenal VCF technically difficult in pregnancy. However, infrarenal VCF was successfully inserted in our patient • Suprarenal VCF offers an easier alternative, however, its potential thrombogenicity with possible renal compromise demand caution with this approach(4) • Conclusions • Retrievable VCF is safe alternative to anticoagulant treatment for pregnant women with increased risk of thromboembolism that are intolerant or for some reasons unsuitable for anticoagulant treatment • It should also be considered in patient with thromboembolism despite adequate anticoagulant treatment • References • 1. Royal College of Obstetricians and Gynaecologists. ‘The Acute Management of Thrombosis and Embolism during Pregnancy and Puerperium’, Green top Guideline No. 37b, London: RCOG Press, 2007 • 2. Cipolla, J. et al (2008) ‘Complications of vena cava filters: A comprehensive clinical review’, OPUS 12 Scientist, vol. 2 (2); pp. 11-24. • 3. Gupta, S., Ettles, D.F., Robinson, G.J., and Lindow, S.W. (2008) ‘Inferior vena cava filter use in pregnancy: preliminary experience’, BJOG, vol. 115 (6); pp. 785-788. • 4. Greenfield, L.J., Cho, K.J., Proctor, M.C., Sobel, M., Shah, S., and Wingo, J. (1992) ‘Late results of suprarenal Greenfield vena cava filter placement’, Arch Surg. 127; pp. 969-973. • Introduction • The risk of thromboembolism is increased significantly in pregnancy. • The risk is further increased in patients with thrombophilia. • Therefore, the use of anticoagulant in pregnancy is mandatory in these patients • Low molecular weight heparin like clexane is the first line anticoagulant in pregnancy (1) • Bleeding complications are rare with the use of clexane in pregnancy (1) • However, when bleeding occurs it pose a management dilemma as in the case report presented. • Retrievable vena cava filters has been found to be a safe alternative as was used in our patient(2,3) • Case Report • The patient is a 33 year old G3P2 (Two previous caeserean sections, last section was 8 years ago) • She is a known thrombophilia (Heterozygous prothrombin gene mutation) with strong positive family history • Her father and brother died of heart attack and pulmonary embolism at the age of 37 and 30 years respectively • She smokes about 10 sticks of cigarrettes a day • Her BMI was 38kg/m2 • She has had three previous episodes of major thromboembolic events. The last episode was a saddle pulmonary embolism 4 years ago (see CTPA showing saddle embolus)