Download
1 / 4

E N D
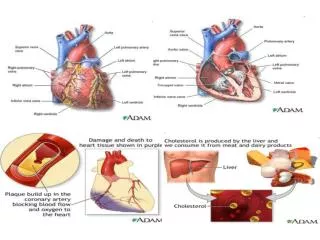
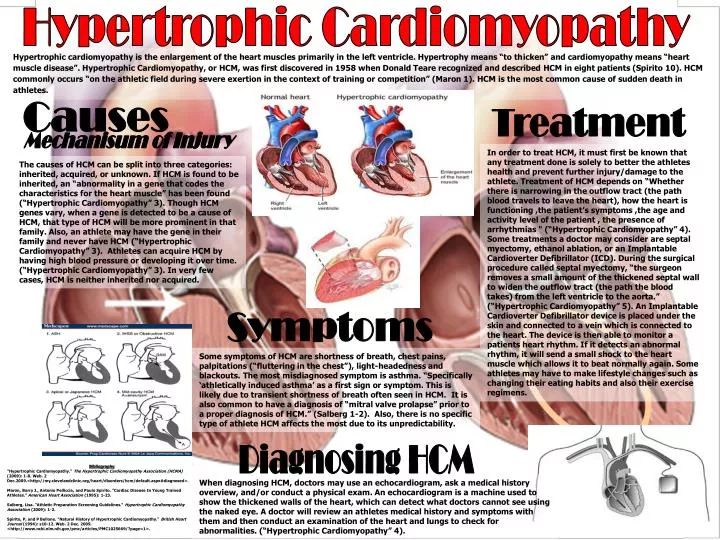
Hypertrophic Cardiomyopathy Hypertrophic cardiomyopathy is the enlargement of the heart muscles primarily in the left ventricle. Hypertrophy means “to thicken” and cardiomyopathy means “heart muscle disease”. Hypertrophic Cardiomyopathy, or HCM, was first discovered in 1958 when Donald Teare recognized and described HCM in eight patients (Spirito 10). HCM commonly occurs “on the athletic field during severe exertion in the context of training or competition” (Maron 1). HCM is the most common cause of sudden death in athletes. Causes Treatment Mechanisum of Injury In order to treat HCM, it must first be known that any treatment done is solely to better the athletes health and prevent further injury/damage to the athlete. Treatment of HCM depends on “Whether there is narrowing in the outflow tract (the path blood travels to leave the heart), how the heart is functioning ,the patient’s symptoms ,the age and activity level of the patient , the presence of arrhythmias " (“Hypertrophic Cardiomyopathy” 4). Some treatments a doctor may consider are septal myectomy, ethanol ablation, or an Implantable Cardioverter Defibrillator (ICD). During the surgical procedure called septal myectomy, “the surgeon removes a small amount of the thickened septal wall to widen the outflow tract (the path the blood takes) from the left ventricle to the aorta.” (“Hypertrophic Cardiomyopathy” 5). An Implantable Cardioverter Defibrillator device is placed under the skin and connected to a vein which is connected to the heart. The device is then able to monitor a patients heart rhythm. If it detects an abnormal rhythm, it will send a small shock to the heart muscle which allows it to beat normally again. Some athletes may have to make lifestyle changes such as changing their eating habits and also their exercise regimens. The causes of HCM can be split into three categories: inherited, acquired, or unknown. If HCM is found to be inherited, an “abnormality in a gene that codes the characteristics for the heart muscle” has been found (“Hypertrophic Cardiomyopathy” 3). Though HCM genes vary, when a gene is detected to be a cause of HCM, that type of HCM will be more prominent in that family. Also, an athlete may have the gene in their family and never have HCM (“Hypertrophic Cardiomyopathy” 3). Athletes can acquire HCM by having high blood pressure or developing it over time. (“Hypertrophic Cardiomyopathy” 3). In very few cases, HCM is neither inherited nor acquired. Symptoms Some symptoms of HCM are shortness of breath, chest pains, palpitations (“fluttering in the chest”), light-headedness and blackouts. The most misdiagnosed symptom is asthma. “Specifically ‘athletically induced asthma’ as a first sign or symptom. This is likely due to transient shortness of breath often seen in HCM. It is also common to have a diagnosis of “mitral valve prolapse” prior to a proper diagnosis of HCM.” (Salberg 1-2). Also, there is no specific type of athlete HCM affects the most due to its unpredictability. Diagnosing HCM Bibliography "Hypertrophic Cardiomyopathy." The Hypertrophic Cardiomyopathy Association (HCMA) (2009): 1-8. Web. 2 Dec.2009.<http://my.clevelandclinic.org/heart/disorders/hcm/default.aspx#diagnosed>. Maron, Barry J., Antonio Pelliccia, and Paulo Spirito. "Cardiac Disease In Young Trained Athletes." American Heart Association (1995): 1-23. Salberg, Lisa. "Athletic Preparation Screening Guidelines." Hypertrophic Cardiomyopathy Association (2009): 1-2. Spirito, P, and P Bellone. "Natural History of Hypertrophic Cardiomyopathy." British Heart Journal (1994): s10-12. Web. 2 Dec. 2009. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1025669/?page=1>. When diagnosing HCM, doctors may use an echocardiogram, ask a medical history overview, and/or conduct a physical exam. An echocardiogram is a machine used to show the thickened walls of the heart, which can detect what doctors cannot see using the naked eye. A doctor will review an athletes medical history and symptoms with them and then conduct an examination of the heart and lungs to check for abnormalities. (“Hypertrophic Cardiomyopathy” 4).
Distal Fracture Radius Distal radius fracture is the most common forearm fracture and is caused by direct impact on the radius, the forearm bone that extends from the lateral side of the elbow to the thumb side of the wrist. It is also known as Colles’ fracture because the Irish surgeon and anatomist Abraham Colles was the first to describe the fracture. [4] Causes Treatment Mechanisum of Injury Wrist fractures and injuries account for 17% of all emergency room visits in the United States. Postmenopausal women with Osteoporosis are at a greater risk to fracture their radius, outnumbering their male counterparts 4:1. A minor fall from standing position can result in a fracture due to the decreased density of the bones. [7] In healthy bones distal radius fractures are the result of “direct impact or axial forces” received after falling onto an outstretched hand (FOOSH). Due to increased involvement in sports, adolescent boys outnumber girls 3:1 in wrist fractures. [2] There are two ways to treat a distal radius fracture: bone re-alignment (reduction) followed by cast immobilization or external fixation. First, the bone is re-aligned to correct the deformity. In closed reduction, the bone is pushed back into place without surgery. In open reduction, surgery is required to re-align the bone and a metal implant is placed on the bone to keep it in place. After, a splint is placed on the forearm and wrist for a few days to aid with normal swelling. Next, a plaster cast is used until replaced by another cast after two to three weeks due to the initial cast loosening from reduction of swelling. The length of placement for the second cast (generally three weeks) is determined by weekly X-rays. [3][6] External fixation devices are used when “fractures are too unstable to treat with a cast.” [1][6] Signs/Symptoms Signs of a distal radius fracture include deformity, bruising, and swelling. Symptoms consist of immediate pain and tenderness. [5] Radius fractures are classified into four categories [5]:intra-articular fracture (fracture extends into the joint) extra-articular fracture (fracture does not extend into the joint) open fracture (fractured bone breaks the skin) comminuted fracture (bone is broken into more than two pieces) Works Cited 1. Geller, Loren, Mitchell Bernstein, Alberto Carli, Greg Berry, Rudy Reindl, and Edward Harvery. "Efficacy of different fixation devices in maintaining an initial reduction for surgically managed distal radius fractures." Canadian Journal of Surgery 52.5 (2009). Gale Group. Web. 17 Nov. 2009. <http://infotrac.galegroup.com/>. 2. Koka, Abid H., Nasser A. Mir, Sohail Majid, and Sahid Najar. "Minimally displaced distal radius fracture: think again!" The Internet Journal of Orthopedic Surgery 11.2 (2009). Gale Group. Web. 17 Nov. 2009. <http://infotrac.galegroup.com/>. 3. Kumar, Prathap, and Seif Sawalha. "Complications of Volar Locking Plates for Distal Radius Fractures: Experience of a District General Hospital." Internet Journal of Orthopedic Surgery (2008). Encyclopaedia Britannica School Edition. Web. 17 Nov. 2009. <http://school.eb.com/>. 4. Lin, Charles, Jui-Sheng Sun, and Sheng-Mou Hou. "External fixation with or without supplementary intramedullary Kirschner wires in the treatment of distal radial fractures." Canadian Journal of Surgery 47.6 (2004). Gale Group. Web. 17 Nov. 2009. <http://infotrac.galegroup.com/>. 5. "Distal Radius Fracture." AAOS - Your Orthopaedic Connection. American Academy of Orthopaedic Surgeons, Aug. 2007. Web. 17 Nov. 2009. <http://orthoinfo.aaos.org/topic.cfm?topic=a00412>. 6. "Distal Radius Fractures, Broken Wrist." DavidLNelson.md. Web. 17 Nov. 2009. <http://www.davidlnelson.md/distalradius.htm>. 7. "Radius, Distal Fractures: eMedicine Radiology." EMedicine - Medical Reference. Web. 17 Nov. 2009. <http://emedicine.medscape.com/article/398406-overview>. Rehabilitation Athletes will begin physical therapy a couple days to weeks after surgery or after the cast is removed. Patients are able to participate in light activities such as swimming and jogging after a month or two after cast removal. Furthermore, a year of recovery is needed to reduce pain and stiffness from vigorous activities. Moderate pain and stiffness continue for another year and fractures from high-energy accidents (automobile collisions, etc.) and Osteoporosis are subjective to permanent stiffness and ache. [5] After surgery, the radius will hurt moderately even after bone reduction. Applying ice, elevating the forearm, and taking non-prescription pain relievers are commonly used to ease the pain. Once the cast is removed, stiffness in the wrist will remain for one to two months. [6]
Orbital Blow Out Fracture An orbital blow-out fracture is a dramatic eye injury in which the maxillary bone or ‘floor’ of the eye socket is fractured. This fracture traps the inferior rectus muscle a muscle that moves the eye ("Orbital). The orbital floor of the eye is made up of the zygomatic and palatine bones in addition to the maxillary (Cohen). Orbital blow-out fractures are commonly caused by a knee, elbow or fist hitting the eye or any blunt trauma to the face and skull (Papouliakos). One-third of orbital fractures occur during contact sports most commonly soccer and boxing (Jones). When the impact occurs, the blow increases pressure in the orbit, causing the weak floor to “blow out” into the maxillary sinus below, trapping the inferior rectus muscle (Widell). The rim of the eye remains intact so the eye is not palpable ("Orbital). Blow-out Fracture injuries require immediate care and management; essential in preventing complications (Karster). Differentiate corrective approaches depend on the severity of the symptoms. * Imaging tests (rate the severity/ entrapment of an eye muscle) * CT scans (fracture site, collection of blood or any displaced tissue). (Colby) Orbital blow-out fractures causes increased pain and swelling due to blood and fluid buildup under the eye, giving the soft tissues overlying the cheekbone a spongy feeling. This swelling may cause the eyelids to swell shut, resulting in visual impairments. Ecchymosis may result in a “black eye” due to the color and the swelling. Double vision can occur if one of the muscles that move the eye is trapped in the fracture (Colby). In other cases, subconjunctival hemorrhages (blood in the whites of the eye) or hyphema (blood inside the eye), may occur. Sources Cohen, Adam J. "Facial Trauma, Orbital Floor Fractures (Blowout): Treatment - eMedicine Plastic Surgery." EMedicine - Medical Reference. Web. 17 Nov. 2009. Colby, Kathryn "Fractures of the Orbit: Injuries to the Eye: Merck Manual Home Edition." Merck & Co., Inc. - We believe the most important condition is the human one. Web. 02 Dec. 2009. "FreeMD." Web. 18 Nov. 2009. <http://www.freemd.com/blowout-fracture-of-the-orbit/evaluation.htm>. Jones, N.P. “Orbital blowout fractures in sport. / fractures orbitales ouvertes en sport.” British Journal of Sports Medicine 28.4 (1994): 272-275. SPORTDiscus with Full Text. EBSCO. Web. 13 Nov. 2009. Karster, PageA., and Craig Yunker "Recognition and Management of an Orbital Blowout Fracture in an Amateur Boxer." Journal of Orthopaedic & Sports Physical Therapy 36.8 (2006): 611-618. SPORTDiscus with Full Text.EBSCO. WEB. 13 Nov. 2009. "Orbital blow-out fracture: Information from Answers.com." Answers.com: Wiki Q&A combined free online dictionary, thesaurus, and encyclopedias. Web. 02 Dec. 2009. Papouliakos, Sotirios M., et al. "Hypoesthesia of the infraobital nerve as the only symptom of a blowout orbital fracture: report of a case and review of the literature.(Case study)." The Internet Journal of Otorhinolaryngology (2007). General OneFile. Web. 3 Nov. 2009. Sabbagh, Leslie. "Timing of surgery is critical." Timing of sugery is critical. 20.45 (1995). Ebsco. Web. Widell, Thomas. "Fracture, Orbital: eMedicine Emergency Medicine." EMedicine Medical Reference. Web. 17 Nov. 2009. Taking incorrect steps in treating patients with orbital fractures can lead to permanent double vision and disfigurements (Sabbagh). Treatment include: *Avoid blowing their nose (can lead to further swelling) *Apply ice (decrease pain and swelling) *Surgery (if needed to repair the facial bones) This is done by restoring bones to their former positions and applying a thing plastic sheet or a bone graft to connect the broken parts (Colby).
Sinus Tarsi Syndrome (STS) is when the space between the talus and calcaneus is injured. The sinus tarsi is an anatomical space bounded by the talus and calcaneus bones. STS was discovered in 1957 by Denis O’Connor. O’Connor also described a surgical procedure call the “O’Connor procedure”. The O’Connor procedure involves the removal of all or just a little section of the sinus tarsi. Other names for this condition include Sinus Tarsi Fat Pad Impingement Syndrome and Sinus Tarsitis. • Diagnostic tools include: • X-Ray • CT Scan • Bone Scan • MRI (preferred method) X-Ray showing the ankle anatomy, specifically the Sinus Tarsi Region • STS usually happens as a complication to an ankle sprain. • Less than 10% of ankle ligament injuries have sinus tarsi syndrome. • Additional causes can include: • Soft tissues in the sinus tarsi being pinched • Repetitive walking or running • Hyperpronation • Signs and symptoms of STS include: • Severe pain in the ankle (specifically in the Sinus Tarsi Region) • Pain during weight-bearing activities (specifically laterally/ outside region) • Ankle instability • Ankle edema (swelling) in the Sinus Tarsi Region • Ankle ecchymosis (bruising) in the Sinus Tarsi Region • STS Treatments may include: • Ice or Heat • Soft tissue massage • Electrotherapy • Joint mobilization • Anti-inflammatory medications • Proper fitting shoes/ orthotics to decrease over pronation • Taping Resistant cases may require cortisone and steroids medication or injections to decrease inflammation and pain. Surgery is rarely needed. Sources: KB, Lee, Bai LB, Song EK, Jung ST et al. Subtalar arthroscopy for sinus Tarsi syndrome: arthroscopic findings and clinical outcomes of 33 consecutive cases. N.p., 28 Oct. 2008. Bouché,, Richard. American Academy of Podiatric Sports Medicine N.p., n.d. Web. 1 Dec. 2009. <http://www.aapsm.org/sinus_tarsi_syndrome.html>. Rinaldi, Robert. Sinus Tarsi Syndrome N.p., 4 June 2008. Web. 1 Dec. 2009. <http://www.vtsports.com/articles/sinus-tarsi-syndrome>. Hermann, M, and KS Pieper. Sinus Tarsi Syndrome: What Hurts? N.p., 11 Feb. 2008. Fluid filling the sinus tarsi (arrow)