Download
1 / 47
490 likes | 842 Vues
Transfusions in Surgery. Dr. Carolyn Faught November 28, 2006. FACT. Approximately 60% of all red cell transfusions are administered to surgical patients Therefore need to understand indications and risks of transfusion. Main Objectives. Be aware of the adverse effects of transfusion

E N D
Transfusions in Surgery Dr. Carolyn Faught November 28, 2006
FACT • Approximately 60% of all red cell transfusions are administered to surgical patients • Therefore need to understand indications and risks of transfusion
Main Objectives • Be aware of the adverse effects of transfusion • Discuss “transfusion triggers” in surgical patients • Treatment of massive transfusion • Indications for recombinant FVIIa in surgical patients
Blood Components • Blood components made by physical separation from whole blood: • Packed red blood cells (PRBCs) • Platelets • Plasma ( FFP, cryoprecipitate) • Granulocytes • Blood derivatives: • Fractioned, virally inactivated product (ie. albumin, IVIG) • Recombinant products (VIII, IX, VIIa)
Universal donor/Universal recipient • Group O RBCs: universal donor, can be given to patients of all blood groups, because no A or B antigens on surface of RBCs • Group AB person is the universal recipient for RBCs, because has no anti-A or anti-B antibodies in plasma • Group AB plasma can be given to all recipients, as it has no anti-A or anti-B antibodies • Emergency (uncrossed) products = O neg RBCs and AB plasma • Still best to give Group specific blood
Blood Products:Universal leukoreduction of all blood products in Canada • ‘third generation’ filters to remove WBCs from blood (leukoreduction) to less than 5x106 WBC/bag of RBCs • Leukoreduction reduces CMV transmission, HLA alloimmunization, febrile non-hemolytic transfusion reactions
Adverse Effects of Transfusion • Transfusion Reactions • Infectious • Non-infectious • Immunologically mediated • Non-immunologic • Immediate • Delayed
Infectious risks of transfusion • Bacterial contamination of platelets 1:40,000* • HBV - 1/250,000 • HIV - 1/1,900,000 • HCV - 1/1,800,000 • HTLV1 - 1/1,000,000 Less clear • CJD (Creutzfeldt-Jakob disease) • West Nile 1/4,000
Non-infectious risks • Febrile reactions • Allergic/anaphylactoid reactions • Hemolytic reactions – 1/20,000 • Volume overload • Acute lung injury (TRALI) • Serologic sensitization • Alloimmunization to red cell antigens (delayed hemolytic transfusion reaction) • Graft-versus host disease • Platelet refractoriness, post-transfusion purpura • Immunomodulation - ? Increased risk of infection, cancer recurrence
TRALI • Transfusion-Related Acute Lung Injury • Non-cardiogenic pulmonary edema after transfusion • Incidence up to 1:5000 transfusions • Antibodies in donor plasma against HLA or neutrophils react with recipient leukocytes • Leukoagglutination in lungs, increase in vascular permeability, fluid enters alveolar spaces • Need to identify, to remove donor from donor pool
TOH Blood Conservation Program • 800 patients a year assessed at Civic • Best candidates are hips, backs, prostate, some gynecologic surgery • Patients assessed 4 wks prior to surgery so they can benefit • Liberal use of Epo and iron • Autologous or 2 unit collection with TRIMA • If Hb > 130 g/L, no Epo • If Hb < 125-130 g/L, no autologous donation
Transfusion Rates Across Canada • Locally, transfusion rates are ~ 45% in hips, 35% in prostate, 25% in knee • Across Canada: • Cardiac: 43.8% female 65% vs male 37% • Hip: 34.4% • ICU (post-op and trauma): 36.9% Can J Anesth 2005: 52(6); 581-590
Transfusion Practices in Surgery • Little evidence to support age-old practice of keeping Hb > 100g/L • General trend towards conservative RBC transfusion practices in elective circumstance • TRICC Trial largest RCT showed RBC transfusion threshold of 70 g/L was as safe as 100 g/L in terms of morbidity and mortality in the critical care setting Hebert, P.C., NEJM 340(6), 1999;409-418
Red blood cell transfusion practices amongst Canadian anesthesiologists: a survey • A threshold above 70 g/L chosen by 48% for general surgery, 56% for orthopedic surgery and 9% for vascular surgery • History of coronary artery disease associated with threshold of 100 g/L • Very young age associated with threshold of </= 60 g/L • Conclusion: general adoption of TRICC trial even in surgical patients Can J Anesth 2006: 53(4); P 344-352
Fresh Frozen Plasma (FFP) • Fresh Frozen Plasma contains the clotting factors necessary for the hemostatic process • Plasma also has volume expansion and oncotic properties • Typical adult dose = 10-20 ml/kg, 4-6 units • Unlikely to be beneficial if PT and/or aPTT <1.5x normal
Massive Transfusion (MT) and Coagulopathy • Definition: replacement of one blood mass in a 24 hour period • More practical definition: transfusion of four or more PRBCs within one hour or replacement of 50% blood volume in three hours • Uncontrolled bleeding causes 40% of deaths in severe trauma
Hemorrhage • Symptoms relate to amount lost • Blood volume (adult) = 75 ml/kg = 5 liters • 10% loss: few symptoms • 20% loss: postural hypotension • 40% loss: shock • 50% loss: irreversible shock
Massive Transfusion and Coagulopathy • Hypothermia – slows activity of coagulation cascade, increases fibrinolysis and alters platelet function • Dilutional coagulopathy – exacerbated by initial volume contraction, fluid resuscitation and transfusion of factor and platelet-deficient PRBCs • Fibrinogen < 1.0 g/L when blood loss 142% • DIC
Disseminated Intravascular Coagulation • Hemostatic defects related to the exaggerated generation of thrombin and fibrin and the excessive consumption of platelets and coagulation factors • Low incidence in elective surgery • In trauma patients: • Due to degree of tissue trauma and tissue anoxia • 40% incidence in brain injury, 25% without head injury
Disseminated Intravascular Coagulation • Incidence of coagulopathy 98% if all of the following: • pH less than 7.10 • Temperature less than 34C • SPB less than 70 mm Hg • Injury severity score greater than 25 Ferrara A, J Trauma 1997;42:857-61
Management of Coagulopathy in MT • PT/PTT increase when factors V, VIII and IX < 50% • Both PT/PTT increased if fibrinogen is low • PT or PTT ratio ≥1.8 means factors are < 30% and leads to high rate of bleeding • No prophylactic regimen of FFP/platelets concentrates has been shown to be effective in MT
Management of Coagulopathy in MT • Correct hypothermia • Correct low Hb – optimum Hb in MT to maintain hemostasis unknown but probably higher than required for O2 delivery • Correct markedly prolonged INR/PTT with FFP ( ratio > 1.5) • Typical use 4-6 units (800-1500 ml) in average adult or 10-20 ml/kg; • gross underestimate in severely depleted, actively bleeding, hypothermic patient and should be 1-1.5:1 ratio of FFP to PRBCs
Management of Coagulopathy in MT • If fibrinogen < 1.0 g/L despite FFP administer cryoprecipitate: 10-20 units • Platelets for decreased platelet count with clinical coagulopathy • Consider rFVIIa if above not sufficient to control bleeding
Recombinant factor VIIa (Niastase) - Background • Recombinant factor VIIa developed to treat hemophilia patients with inhibitors • By-passing agent in patients not responding to factor replacement • Recombinant factor VIIa used for treatment and prophylaxis of hemophiliacs with inhibitors • Use expanded to other bleeding patients
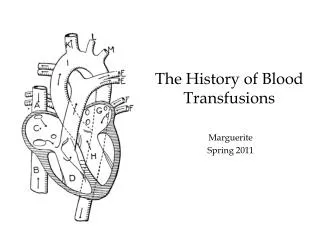
II Xa IIa Factor VIIa in Normal Hemostasis X VIII/vWF TF VIIa Va VIIIa TF-Bearing Cell TF V Va VIIa IX Platelet II IXa X Xa IIa VIIIa IXa Va FibrinClot Activated Platelet VIIa IXa Va VIIIa IIa Xa II IX X Hoffman M, et al. Blood Coagul Fibrinolysis. 1998;9(suppl 1):S61-S65.
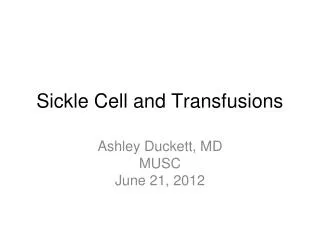
FVIIa – FVIII and FIX Independant II X TF VIIa Xa IIa Va TF-Bearing Cell TF V Va Platelet II X FibrinClot VIIa Xa IIa Va Activated Platelet Hoffman M, et al. Blood Coagul Fibrinolysis. 1998;9(suppl 1):S61-S65.
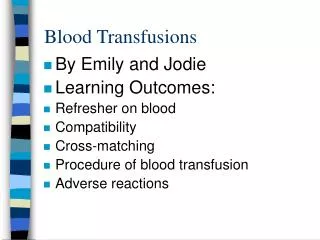
High-Dose FVIIa Enhances IIa Generation Without TF 4 Normal Hemophilic 3 Relative IIa generation 2 1 0 0 1 10 100 [FVIIa] (nM) Monroe DM, et al. BrJ Haematol 1997;99:542-547.
Niastase: Licensed Indications • Treatment of bleeding in hemophilia patients with inhibitors • Surgical management of hemophilia patients with inhibitors • Congenital factor VII deficiency (USA) • Glanzmann’s Thrombasthenia (UK)
Pharmacology of Recombinant Factor VIIa • 50,000 MW molecule with t ½ of 2 hrs • Normal concentration of factor VII: 10-20 nm • 1% of factor VII circulates in activated form • Standard dose in hemophilia 90 ug/kg • maximum concentration 50 nm • 500 x normal concentration of VIIa • Dosing q 2-3 h to maintain hemostatic levels
Expanded Use of VIIa • Factor VII deficiency • Other factor deficiencies (FXI, acquired FX) • Von Willebrand’s disease • Thrombocytopenia • Platelet function defects • Reversal of oral anticoagulation • Coagulopathy of liver disease • Surgical bleeding • Surgical prophylaxis • Intracranial hemorrhage • Trauma
VIIa in Partial Hepatectomy: Placebo Controlled RCT Design: • RCT comparing 20, 80 ug/kg or placebo in non-cirrhotic patients with 2nd dose for OR > 6 hrs • Monitored for bleeding for 7 days Results: • 185 patients Lodge et al. Hepatology 2002;36:Abst177
VIIa in Partial Hepatectomy Placebo 20 ug/kg 80ug/kg Blood loss 1000 800 700 % transfused 37% 41% 25% Thrombosis 3 3 3 Trend but no significant difference
Effect of rVIIa on Perioperative Blood Loss During Prostatectomy Friederich. Lancet 2003 Design • 36 pts randomized to placebo or rVIIa (20 ug/kg or 40 ug/kg) • Followed for 10 days post-op Results
RecombinantVIIa for Adjunctive Hemorrhage Control in Trauma Patients • 7 patients with coagulopathic bleeding treated under compassionate use program • Age 17-75 • No atherosclerosis/thromboembolic disease • Received 20-70 units RBCs + FFP and platelets Intervention • 1-3 doses of 60-120 ug/kg of rVIIa Matinowitz et al. J Trauma 2001;51:431
Recombinant VIIa for Adjunctive Hemorrhage Control in Trauma Results • Bleeding stopped/reduced in all patients • Further transfusions limited to 1-2 units of RBCs • Significant shortening of coagulation tests • 4 of 7 patients survived • No thrombotic events
Multicentre RCT of rVIIa in Trauma • 280 pts with blunt or penetrating trauma • All patients receive 3 doses • 200 ug/kg followed by 100ug/kg 1h and 3h later Arrive at ER rVIIa 48h 30d trauma randomize 0 6 8 placebo Units of RBCs 48h 30d Transfusion ICU/Hosp LOS Survival Adverse Events Boffard et al. J Trauma. 2005: 59: 8-15
Multicentre RCT of rVIIa in Trauma • Non significant reduction in RBC units transfused • Significant reduction in RBC units (2.6 units) and incidence of massive transfusion (14% vs 33%) in blunt trauma when early deaths excluded • Similar overall survival - 25% vs 30% • Composite outcome incl organ dysfunction showed increased trend favouring rVIIa (29 vs. 43%) • No difference in adverse events Boffard et al. J Trauma. 2005: 59: 8-15
Complications Associated with Factor VIIa FDA report of adverse events from trials and voluntary reporting from 1999-2005 • 220 thromboembolic complications • 193 in non-hemophiliac patients • 129 arterial thrombosis • 103 venous thrombosis • Approx. 50% of reports within 24 hrs of infusion • 43 of 67 deaths reported secondary to thrombosis