Download
1 / 45
620 likes | 2.16k Vues
Superior Sulcus Tumors. Clinical Evaluation and Staging. Benan Çağlayan Dr.Lütfi Kırdar Kartal Training and Research Hospital. 1924 Pancoast Shoulder and arm pain along the distribution of C8 – T2 nerve roots Horner’s syndrome Weakness and atrophy of the muscles of the hand

E N D
Superior Sulcus Tumors Clinical Evaluation and Staging Benan Çağlayan Dr.Lütfi Kırdar Kartal Training and Research Hospital
1924 Pancoast • Shoulder and arm pain along the distribution of C8 – T2 nerve roots • Horner’s syndrome • Weakness and atrophy of the muscles of the hand • 1932 Pancoast & Tobias • Bronchogenic carcinoma
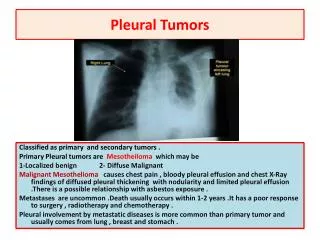
Superior Sulcus Tumor • SS tumors arise in the apex of the lung • Parietal pleura • Endothoracic facia • Subclavian vessels • Brachial plexus • Adjacent ribs and vertebral column • Stellate ganglion can be invased
Definition • Any tumor localised at the typical pancoast tumor location (without Horner’s syndrome and pain) • The tumor originating from apices of the lung and invasing apical thoracal structures • Chest wall, vertebrae, subclavian vessel • Apical tumor + Pancoast syndrome • The tumor originating from posterior apical part of the upper lobe which causes symptoms related to C8, T1, T2 nerve roots involvement (with / without Horner’s syndrome) • The tumor invasing apical chest wall structures • İnfiltration of the chest wall at the level of the second rib or lower, or of the visceral pleura only, is not considered as SST • Chest wall invasion limited to parietal pleura only can be considered as SST
Presentation • Shoulder and arm pain • Pancoast Syndrome • Shoulder pain • Pain of the medial aspect of the arm and hand (ulnar distiribution) • Paresthesia, weakness and atrophy of the medial aspect of the arm and hand • Paresthesia and pain of the 4th and 5th digits • Horner’s syndrome (14 -50%) • Ptosis, miosis, anhidrosis • Ipsilateral flushing and hyperhidrosis of the face • Reflex symphathetic dystrophy • Due to invasion of upper part of the thoracic symphathetic trunk • Burning, oedema, eritema, warming and tenderness of the extremity
With further extension through the intervertebral foramina • Paraplegia or quadroplegia • In 5% of the patients initially • In 25 % of the patients later in the course of the disease
Frank C. Detterbeck. Changes in the treatment of Pancoast tumors. Ann Thorac Surg 2003;75:1990-7
Rare symptoms and signs • Supraclavicular LAM • SVCS • Involvement of the phrenic and recurrent laryngeal nerves • Pulmonary symptoms: Cough, dyspnea, haemopthysis
Tumor Biology • Local invasion rather than lymphatic and hematogenous metastasis ? • pN2 10 – 20% • Survival is better with lobectomy compared to segmentectomy
< 5 % of all lung cancer cases • Non-Small Cell Lung Cancer • Squamous Cell Ca*** • Adeno Ca** • Large Cell Ca* • Small Cell Lung Cancer % 1
Diagnosis • Characteristic pain • Chest X Ray • Unilateral apical cap > 5mm • Bilateral asymetric apical cap • Apical mass • Bone destruction
Thoracic CT • In addition to the apical mass • Invasion of chest wall, vertebrae and vessel • Other pulmonary nodule(s), parenchymal diseases • Mediastinal evaluation • Helps to choose which way is better in diagnosis and staging • Adrenal glands must be included • MDCT has advantage of multiplaner reformatting
No ionizing radiation The ability to image in any plane The neural foramina is better visualized Helps to differentiate the diagnosis of relaps and radiation fibrosis Thoracic MRI The anatomical structures above the apex are better visualized with coronal and sagittal planes (Brachial plexus, vessels)
Histologic diagnosis • Cytologic analysis of sputum 10 – 20 % • Bronchoscopy • Martinod: 13.7 % • Alifano: 13.4 % • Wright : 0 % • Sartori: 29.8 % • Scalene node / subscalene biopsy • Percutaneous FNA / tru cut biopsy 95 % • Giuliano: 96.4 % • VATS / Thoracotomy
Staging Mountain C. Chest 1997; 111:1710-1717
MX : Present of distant metastasis cannot be assessed M0: No distant metastasis M1: Distant metastasis present Mountain C. Chest 1997; 111:1710-1717
Non invasive staging History, physicial examination Chest X-Ray Abdominal USG Bone scanning Cranial CT / MRI Thoracic CT – Upper abdominal CT Thoracic MRI Angiography PET PET – CT EMG Invasive staging C.Mediastinoscopy(1,2, 4,7A) Anterior mediastinotomy( APW) EUS-NA (5, 7, 8, 9) TBNA EBUS-NA TTNA VATS Staging
History – Physical examination • Pancoast syndrome (T4) • Horner’s syndrome (T3) • Clinical findings of haematogeneous metastasis (M1)
Staging • Chest X-Ray • Bone destruction • Bulky LN • Pleural effusion • Pulmonary nodul(s) within the ipsilateral but other than primary tumor lobe or contralateral lung
Staging • Thoracic CT • First step to evaluate the nature of the lesion and to diagnose lung cancer • Unexpensive and easily available • With history and physical examination findings it puts forward the need for PET or other staging modalities • Technical availability and feasibility of invasive staging modalities depend on anatomical characteristics of lesions (not metabolic)
Chest wall invasion • Thoracic CT • Sensitivity with 38-87 % and specificity with 40-90 % • Costal destruction • Pleural thickening • Obliteration of extrapleural fat plane • Contact with chest wall in a wide angle • More than 3 cm contact with chest wall • With artificial pneumothorax; sensitivity 100 % and specificity 57-80 %
Chest wall invasion • Thoracic MRI • The extent of chest wall invasion adjacent to a lung tumor may be better shown by using MRI than CT because of better contrast on T1- and T2-weighted images between tumor and chest wall fat and muscle • Chest wall invasion is best depicted as a disruption of the extrapleural fat line • Haggar et al. NPV 100 % • Padovani; sensitivity 90 %, specificity 86 % • Involvement of the subclavian vessels, brachial plexus, vertebral body, neural foramina and lung apices are better shown on coronal and sagittal MRI
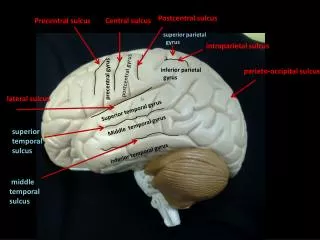
Brachial plexus invasion • Brachial plexus is better oriented to coronal plane • Axial plane better visualizes the proximal part, sagittal plane better visualizes the distal part of brachial plexus
Brachial plexus invasion • Nervous tissue can be better visualized • Each and every nerve can be differentiated from adjacent vascular structures and soft tissue • As Brachial plexus is relatively fixed structure, less image degradation while breathing • It is possible to differentiate the mass from not only Brachial plexus but also adjacent soft tissue
Superior sulcus invasion Heelan RT et al. Superior sulcus tumors:CT and MR imaging. Radiology 1989;170:637-641
MDCT • High quality spiral CT with thin section, bolus injection of contrast agents and sagittal and coronal reformats provides the same information • MRI may be reserved for patients with extension into the neural foramina and the epidural space
Other staging modalities • EMG and neurologic examination • Clarify invasion to Brachial plexus and phrenic nerve and epiduritis • In case of suspicion of vascular invasion • MR anjiography • Venous anjiography • Subclavian arteriography • Cervical doppler USG
T3 Tumor • Parietal pleura • Sympathetic chain • Stellate ganglion (Horner’s synd.) • Azygos vein • Vertebrae • İnvasion of processus • transversus? • Radiologically no verteb- • ral erosion, with only inva- • sion of adjacent soft tissue • (pleura, prevertebral facia • and periosteum) • Brachial plexus • T1 root invasion only • T4 Tumor • Mediastinal invasion • Invasion of vertebrae • Corpus or costo-transvers • foramina • Confirmed periostal invasion in • resected specimen • Invasion of Brachial plexus • Pancoast synd. (Horner’s • synd. +C8-T1 + muscle atrophy) • Invasion of Subclavian vessels
Nodal staging - CT • Mediastinal lymph node involvement is the most important prognostic factor and influences therapeutic strategies. • A diameter larger than 1cm in the short axis is generally considered as the standard criterion for a suspicious LN • Contrast CT is very accurate in detecting LN enlargement • Small nodes may contain metastasis in up to 20% • Large nodes may be benign (40%) • Cervical mediastinoscopy is recommended even in case of LN < 1 cm, if curative resection is planned for SST
Nodal staging - CT • According to total of 43 studies including 5111 patients • Sensitivity 51%, specificity 86% • Helps to decide which of TBNA,TTNA, mediastinoscopy / tomy, VATS should be used Noninvasive staging of NSCLC. ACCP evidence-based clinical practice guidelines (2nd Edition) Chest 2007;132:178-201s
Nodal staging – PET scanning • Based on the metabolic activity • Standart uptake value (SUV) > 2.5 • PET-CT • PET: Biological visualization • CT: Anatomical visualization • Between 1994 – 2006 studies including 2865 patients showed • Sensitivity 74% • Specificity 85%
Nodal staging – PET scanning • Non-invasive lung cancer staging was substantially improved by the use of PET • PET is superior to CT for mediastinal LN staging in potentially operable NSCLC • PET correctly icreased or decreased nodal staging as determined by CT in 25% in pre-surgical patients • Sensitivities and negative predictive values (NPVs) were comparable for PET compared with mediastinoscopy • In case of positive mediastinal PET, tissue confirmation is still needed to confirm LN metastasis
Advantages • Whole body scanning • No need for bone scanning and abdominal CT • Unexpected metastasis can be diagnosed (20%) • Biologically active lymph node make guideness for invasive procedure • Disadvantages • In case of falce positiveness patients might loose the chance of operation
Nodal staging - Endoscopy • TBNA • An operator depended procedure and the positivity is corralated with the size of lymph node • With its high PPV it can be recommended as initial staging procedure. In case of negativitiy mediastinoscopy / tomy should be performed • EBUS • EEUS-NA • TTNA • CT guided • Generally used for bulky lymph nodes • Anterior parasternal approach for 1,2,4,5 and 6th stations • Posterior paraspinal approach for 4,7,8 and 9th stations
Nodal staging - Mediastinoscopy • Mediastinoscopy remains the gold standard for invasive staging of patients with potentially operable lung cancer. • The highest mediastinal LN station , • The right and left superior paratracheal LN stations , • The right and left inferior paratracheal LN stations , • And the subcarinal LN station
Performance of different locoregional staging techniques Sensitivity (%)Specificity (%)NPV (%)PPV (%)Prevalence (%) CT 57 82 83 56 28 PET 84 89 93 79 32 Blind TBNA 76 96 71 100 70 EEUS-FNA 88 91 77 98 69 Mediastinoscopy 81 100 91 100 37 Preoperative lymph node staging for non-small cell lung cancer. ESTS guidelines P. De Leyn, D. Lardinois, P. Van Schil, R. Rami-Porta, B. Passlick, M. Zielinski, D. Waller,
Features of a standadized evaluation for systemic metastases Noninvasive staging of NSCLC. ACCP evidence-based clinical practice guidelines (2nd Edition) Chest 2007;132:178-201s
Recommendations • In patients with a Pancoast tumor, it is recommended that a tissue diagnosis be obtained before initiation of therapy (1C) • In patients who have Pancoast tumor and are being considered for curative intent surgical resection, an MRI of the thoracic inlet and brachial plexus is recommended to rule out tumor invasion of unresectable vascular structures or the extradural space (1C). • In patients who have Pancoast tumor and are being considered for curative resection, invasive mediastinal staging and extrathoracic imaging (head CT/MRI plus either whole-body PET or abdominal CT plus bone scan) are recommeded. Involvement of mediastinal nodes and/or metastatic disease represent a contrindication to resection (1C). Special treatment issues in lung cancer. ACCP evidence-based clinical pratice guidelines (2nd Edition) Chest 2007;132:290-305s