Download
1 / 1
10 likes | 171 Vues
CANNABIS AND SCHIZOPHRENIA SALİH YAŞAR ÖZDEN MD, MELTEM SEVİM MD, E. MÜJGAN ÖZEN ŞAHİN MD BAKIRKÖY MENTAL HOSPITAL, İSTANBUL/TURKEY.

E N D
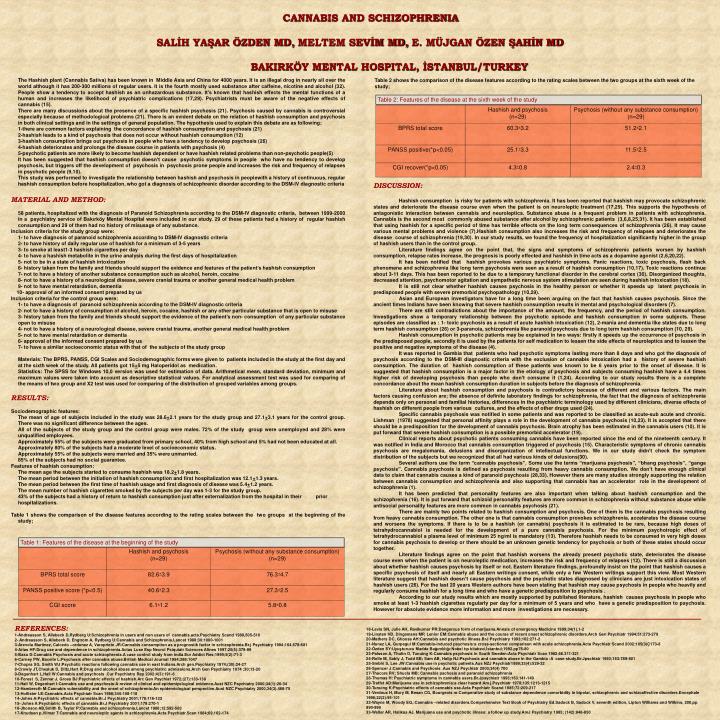
CANNABIS AND SCHIZOPHRENIA SALİH YAŞAR ÖZDEN MD,MELTEM SEVİM MD,E. MÜJGAN ÖZEN ŞAHİN MD BAKIRKÖY MENTAL HOSPITAL, İSTANBUL/TURKEY The Hashish plant(Cannabis Sativa) has been known in Middle Asia and China for 4000 years. It is an illegal drog in nearly all over the world although it has 200-300 millions of regular users. It is the fourth mostly used substance after caffeine, nicotine and alcohol (32). People show a tendency to accept hashish as an unhazardous substance. It’s known that hashish effects the mental functions of a human and increases the likelihood of psychiatric complications (17,29). Psychiatrists must be aware of the negative effects of cannabis (15). There are many discussions about the presence of a specific hashish psychosis (21). Psychosis caused by cannabis is controversial especially because of methodological problems (21). There is an evident debate on the relation of hashish consumption and psychosis in both clinical settings and in the settings of general population. The hypothesis used to explain this debate are as following; 1-there are common factors explaining the concordance of hashish consumption and psychosis (21) 2-hashish leads to a kind of psychosis that does not occur without hashish consumption (12) 3-hashish consumption brings out psychosis in people who have a tendency to develop psychosis (26) 4-hashish deteriorates and prolongs the disease course in patients with psychosis (4) 5-psychotic patients are more likely to become hashish dependent or have hashish related problems than non-psychotic people(5) It has been suggested that hashish consumption doesn’t cause psychotic symptoms in people who have no tendency to develop psychosis, but triggers off the development of psychosis in psychosis prone people and increases the risk and frequency of relapses in psychotic people (9,10). This study was performed to investigate the relationship between hashish and psychosis in peoplewith a history of continuous, regular hashish consumption before hospitalization, who got a diagnosis of schizophrenic disorder according to the DSM-IV diagnostic criteria MATERIAL AND METHOD: 58 patients, hospitalized with the diagnosis of Paranoid Schizophrenia according to the DSM-IV diagnostic criteria, between 1999-2000 in a psychiatry service of Bakırköy Mental Hospital were included in our study. 29 of these patients had a history of regular hashish consumption and 29 of them had no history of misusage of any substance. Inclusion criteria for the study group were: 1- to have diagnosis of paranoid schizophrenia according to DSM-IV diagnostic criteria 2- to have history of daily regular use of hashish for a minimum of 3-5 years 3- to smoke at least1-3 hashish cigarettes per day 4- to have a hashish metabolite in the urine analysis during the first days of hospitalization 5- not to be in a state of hashish intoxication 6- history taken from the family and friends should support the evidence and features of the patient’s hashishconsumption 7- not to have a history of another substance consumption such as alcohol, heroin, cocaine 8- not to have a history of a neurological disease, severe cranial trauma or another general medical healthproblem 9- not to have mental retardation, dementia 10- approval of an informed consent prepared by us Inclusion criteria for the control group were; 1- to have a diagnosis of paranoid schizophrenia according to the DSM-IV diagnostic criteria 2- not to have a history of consumption of alcohol, heroin, cocaine, hashish or any other particular substance that is open to misuse 3-history taken from the family and friends should support the evidence of the patient’s non- consumption of anyparticular substance open to misuse 4-not to have a history of a neurological disease, severe cranial trauma, another general medical health problem 5- not to have mental retardation or dementia 6-approval of the informed consent prepared by us 7- to have a similar socioeconomic status with that of the subjects of the study group Materials: The BPRS, PANSS, CGI Scales and Sociodemographic forms were given to patients included in the study at the first day and at the sixth week of the study. All patients got 15+5 mg Haloperidol as medication. Statistics: The SPSS for Windows 10,0 version was used for estimation of data. Arithmetical mean, standard deviation, minimum and maximum values were taken into account as descriptive statistical values. For analytical assessment test was used for comparing of the means of two group and X2 test was used for comparing of the distribution of grouped variables among groups. RESULTS: Sociodemographic features: The mean of age of subjects included in the study was 28.6+2.1 years for the study group and 27.1+3.1 years for the control group. There was no significant difference between the ages. All of the subjects of the study group and the control group were males. 72% of the study group were unemployed and 28% were unqualified employees. Approximately 55% of the subjects were graduated from primary school, 40% from high school and 5% had not been educated at all. Approximately 80% of the subjects had a moderate level of socioeconomic status. Approximately 55% of the subjects were married and 35% were unmarried. 85% of the subjects had no social guarantee. Features of hashish consumption: The mean age the subjects started to consume hashish was 18.2+1.8 years. The mean period between the initiation of hashish consumption and first hospitalization was 12.1+1.3 years. The mean period between the first time of hashish usage and first diagnosis of disease was 5.4+1.2 years. The mean number of hashish cigarettes smoked by the subjects per day was 1-3 for the study group. 43% of the subjects had a history of return to hashish consumption just after externalization from the hospital in their priorhospitalizations. Table 1 shows the comparison of the disease features according to the rating scales between the two groups at the beginning of the study; Table 2 shows the comparison of the disease features according to the rating scales between the two groups at the sixth week of the study; Table 2: Features of the disease at the sixth week of the study DISCUSSION: Hashish consumption is risky for patients with schizophrenia. It has been reported that hashish may provocate schizophrenic states and deteriorate the disease course even when the patient is on neuroleptic treatment (17,29). This supports the hypothesis of antagonistic interaction between cannabis and neuroleptics. Substance abuse is a frequent problem in patients with schizophrenia. Cannabis is the second most commonly abused substance after alcohol by schizophrenic patients (3,6,8,25,31). It has been established that using hashish for a specific period of time has terrible effects on the long term consequences of schizophrenia (26). It may cause various mental problems and violence (7).Hashish consumption also increases the risk and frequency of relapses and deteriorates the disease course of schizophrenia (19,30). In our study results, we found the frequency of hospitalization significantly higher in the group of hashish users than in the control group. Literature findings agree on the point that, the signs and symptoms of schizophrenic patients worsen by hashish consumption, relapse rates increase, the prognosis is poorly effected and hashish in time acts as a dopamine agonist (2,6,20,22). It has been notified that hashish provokes various psychiatric symptoms. Panic reactions, toxic psychosis, flash back phenomena and schizophrenia like long term psychosis were seen as a result of hashish consumption (10,17). Toxic reactions continue about 3-11 days. This has been reported to be due to a temporary functional disorder in the cerebral cortex (30). Disorganized thoughts, decreased attention, psychomotor agitation and sympathetic nervous system stimulation are seen during hashish intoxication (18). It is still not clear whether hashish causes psychosis in the healthy person or whether it speeds up latent psychosis in predisposed people with severe premorbid psychopathology (10,29). Asian and European investigators have for a long time been arguing on the fact that hashish causes psychosis. Since the ancient times Indians have been knowing that severe hashish consumption results in mental and psychological disorders (7). There are still contradictions about the importance of the amount, the frequency, and the period of hashish consumption. Investigations show a temporary relationship between the psychotic episode and hashish consumption in some subjects. These episodes are classified as : 1- toxic psychosis as a result of acute hashish intoxication (12), 2-mania and dementia like states due to long term hashish consumption (26) or 3-paranoia, schizophrenia like paranoid psychosis due to long term hashish consumption (10, 29). Hashish consumption in psychotic patients may be explained in two ways: firstly it speeds up the occurrence of psychosis in the predisposed people, secondly it is used by the patients for self medication to lessen the side effects of neuroleptics and to lessen the positive and negative symptoms of the disease (4). It was reported in Gambia that patients who had psychotic symptoms lasting more than 8 days and who got the diagnosis of psychosis according to the DSM-III diagnostic criteria with the exclusion of cannabis intoxication had a history of severe hashish consumption. The duration of hashish consumption of these patients was known to be 6 years prior to the onset of disease. It is suggested that hashish consumption is a major factor in the etiology of psychosis and subjects consuming hashish have a 4.4 times higher risk of developing psychosis than people who don’t consume it (1,24). According to our study results there is a complete concordance about the mean hashish consumption duration in subjects before the diagnosis of schizophrenia. Literature about hashish consumption and psychosis is contradictory because of different and various factors. The main factors causing confusion are; the absence of definite laboratory findings for schizophrenia, the fact that the diagnosis of schizophrenia depends only on personal and familial histories, differences in the psychiatric terminology used by different clinicians, diverse effects of hashish on different people from various cultures, and the effects of other drugs used (24). Specific cannabis psychosis was notified in some patients and was reported to be classified as acute-sub acute and chronic. Lishman (1978) suggested that personal affinity plays a role in the development of cannabis psychosis (10,23). It is accepted that there should be a predisposition for the development of cannabis psychosis. Brain atrophy has been estimated in the cannabis users (10). It is put forward that severe hashish consumption is a possible premorbid accelerator (19). Clinical reports about psychotic patients consuming cannabis have been reported since the end of the nineteenth century. It was notified in India and Morocco that cannabis consumption triggered of psychosis (15). Characteristic symptoms of chronic cannabis psychosis are megalomania, delusions and disorganization of intellectual functions. We in our study didn’t check the symptom distribution of the subjects but we recognized that all had various kinds of delusions(30). Several authors use the term “cannabis psychosis”. Some use the terms “marijuana psychosis”, “bhang psychosis”, “ganga psychosis”. Cannabis psychosis is defined as psychosis resulting from heavy cannabis consumption. We don’t have enough clinical data to claim that cannabis causes a kind of paranoid psychosis (28,33). However there are many studies strongly supporting the relation between cannabis consumption and schizophrenia and also supporting that cannabis has an accelerator role in the development of schizophrenia (1). It has been predicted that personality features are also important when talking about hashish consumption and the schizophrenia (16). It is put forward that schizoid personality features are more common in schizophrenia without substance abuse while antisocial personality features are more common in cannabis psychosis (21). There are mainly two points related to hashish consumption and psychosis. One of them is the cannabis psychosis resulting from heavy cannabis consumption. The other one is that cannabis consumption provokes schizophrenia, accelerates the disease course and worsens the symptoms. If there is to be a hashish (or cannabis) psychosis it is estimated to be rare, because high doses of tetrahydrocannabiol is needed for the development of a pure cannabis psychosis. For the minimum psychotropic effect of tetrahydrocannabiol a plasma level of minimum 25 ng/ml is mandatory (13). Therefore hashish needs to be consumed in very high doses for cannabis psychosis to develop or there should be an unknown genetic tendency for psychosis or both of these states should occur together. Literature findings agree on the point that hashish worsens the already present psychotic state, deteriorates the disease course even when the patient is on neuroleptic medication, increases the risk and frequency of relapses (12). There is still a discussion about whether hashish causes psychosis by itself or not. Eastern literature findings, profoundly insist on the point that hashish causes a specific psychosis of itself and nearly all Eastern writings consent, while only a few Western writings support this view. Most Western literature suggest that hashish doesn’t cause psychosis and the psychotic states diagnosed by clinicians are just intoxication states of hashish users (26). For the last 20 years Western authors have been stating that hashish may cause psychosis in people who heavily and regularly consume hashish for a long time and who have a genetic predisposition to psychosis . According to our study results which are mostly supported by published literature, hashish causes psychosis in people who smoke at least 1-3 hashish cigarettes regularly per day for a minimum of 5 years and who have a genetic predisposition to psychosis. However for absolute evidence more information and more investigations are necessary. Table 1: Features of the disease at the beginning of the study 18-Levis SN, Julie AH, Ravikumar PR:Dangerous form of marijuana.Annals of emergency Medicine 1999;34(1).1-2 19-Linsten HD, Dingemans MP, Lenior EM:Cannabis abuse and the course of recent onset schizophrenic disorders.Arch Gen Psychiatr 1994;51:273-279 20-Mathers DC, Ghoose AH:Cannabis and psychotic illness.BrJ Psychiatry 1993;162:271-2 21-Nunez LA, Gurpegui M:Cannabis-induced psychosis:a cross-sectional comparison with acute schizophrenia.Acta Psychiatr Scand 2002;105(3)Ç173-8 22-Özden SY:Uyuşturucu Madde Bağımlılığı:Nobel tıp kitabevi,İstanbul;1992.pp76-80 23-Palsson A, Thulin O, Tunuing K:Cannabis psychosis in South Sweden:Acta Psychiatr Scan 1982;66.311-321 24-Rolfe M, Sably J, Todd EB; Sam AB, Hatip NJ:Psychosis and cannabis abuse in the Gambia :A case study.Br.Jpschiatr 1993;163:789-801 25-Smbhi S, Lee JW:Cannabis use in psychotic patients.Aus NZJ Psychiatr1999;33(4):529-32 26-Spencer J:Cannabis and Psychosis .Aus NZJ Psychiatr 2000;34(4) 700 27-Thacore RV; Shucla MB: Cannabis pschosis and paranoid schizophrenia 28-Thomas H: Psychiatric symptoms in cannabis users.Br.Jpsychiatr 1993;163.141-149 29-Treffet AD:Marijuana use in schizophrenia:a clear hazard:Am.j.Psychiatr 1978;135:1213-1215 30-Tunuing K:Psychiatric effects of cannabis use.Acta Psychiatr Scand 1985;72:209-217 31-Verdoux H, Mury M, Besan CG, Bourgeois m:Comperative study of substance dependence comorbidity in bipolar, schizophrenic and schizoaffective disorders.Encephale 1996;22(2):95-101 32-Wayne M, Woody EG,:Cannabis –related disorders.Comprehensive Text Book of Psychiatry Ed.Sadock B, Sadock V, seventh edition, Lipton Williams and Wilkins, 200,pp 990-999 33-Weller AR, Halikas AJ. Marijuana use and psychotic illness: a follow up study.AmJ Psychiatry 1985; (142):848-850 REFERENCES: 1-Andreasson S, Allebeck D,Rydberg U:Schizophrenia in users and non users of cannabis.acta.Psychiatry Scand 1989,505-510 2- Andreasson S, Allebeck D, Engtrom A, Rydberg U:Cannabis and Schizophrenia.Lancet 1988;30:1000-1001 3-Arevola Martinez, Calcedo –ordonez A, Varoprieto JR:Cannabis consumption as a prognostik factor in schizophrenia.Br.j Psychiatry 1994;164.679-681 4-Arias HF:Drug use and dependence in schizophrenia.Actas Luse Esp Neurol Psiquiatr Sciences Afines 1997;25(6):379-89 5-Basu D:Cannabis Psychosis and acute schizophrenia.A case control study from india.Eur Addict Res;1999;5(2):71-3 6-Carney PW, Bacelle L:Psychosis after cannabis abuse.British Medical Journal 1984;288:1047 7-Chopra SG, Smith WJ:Psychotic reactions following cannabis use in east Indians.Arch gen.Psychiatry 1974;(30):24-27 8-Crowly JT,Chesluk D, Diltz,Hart R:Drug and alcohol abuse among psychiatric admissions.Arch Gen Psychiatry 1974 ;30;13-20 9-Degenhart L,Hall W:Cannabis and psychosis .Cur Psychiatry Rep 2002;4(3):191-6 10-Forest S, Zennar J, Groes BJ:Psychiatric effects of hashish.Arc Gen Psychiat 1972;(27):133-138 11-Hall W, Degenhart l:Cannabis use and psychosis:A review of clinical and epidemiyological evidence.Aust NZC Psychiatry 2000;34(1):26-34 12-Hambrecth M:Cannabis vulnerability and the onset of schizophrenia:An epidemiological perspective.Aust NZC Psychiatry 2000,34(3).468-75 13-Hollister LE:Cannabis.Acta Psychiatr Scan 1988;345:108-118 14-Johns A:Psychiatric effects of cannabis.Br.J Psychiatry 2001;178:116-122 15- Johns A:Psychiatric effects of cannabis.Br.J Psychiatry 2001;179:270-1 16-Jhonson AB,Smith B, Taylor P:Cannabis and schizophrenia.Lancet 1988;12:592-583 17-Knudsen p,Vilmar T:Cannabis and neuroleptic agents in schizophrenia.Acta Psychiatr.Scan 1984;69.162-174