Download
1 / 26
330 likes | 2.78k Vues
Thermoregulation in infants and newborn. Dr.Ayman Ibrahim Tharwat M.D. Temperature regulation. Normal thermoregulation in infants and children: Physiologic mechanisms:

E N D
Thermoregulation in infants and newborn Dr.Ayman Ibrahim Tharwat M.D
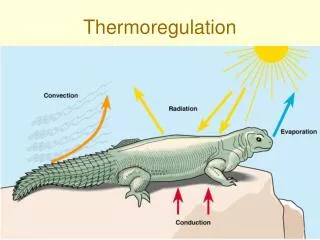
Temperature regulation Normal thermoregulation in infants and children: • Physiologic mechanisms: • Intraoperative hypothermia provokes peripheral vasoconstriction, the principal site for thermoregulation is the hypothalamus. • The hypothalamus interprets signals from other parts of the body, the spinal cord, the central core tissues, and the skin surface.
Temperature regulation • The processing of the thermoregulation occurs in three stages: Afferent thermal sensing: In the periphery, anatomically distinct cold and warm receptors detect the ambient temperature ,send impulses through A delta fibers and C fibers along the spinothalamic tract in the anterior spinal cord.
Central regulation: • When the integrated input from all the sources exceeds the upper threshold or fall bellow the lower threshold, thermoregulation occurs. • The interthreshold range through which no regulation occurs is wider during anesthesia (3.5c) than during normal circumstances (0.2c), The interthreshold range is also wider in the hypothermic state than in the hyperthermic state.
Efferent responses: • Thermal deviations from the threshold temperature initiate efferent responses that increase metabolic responses (non shivering and shivering responses), decrease environmental heat loss (active vasodilatation, sweating, behavioral responses which is the most important) . • Cutaneous vasoconstriction is the first and most consistent thermoregulatory response to hypothermia. The ability to produce heat by increasing metabolic rate and oxygen consumption is the other component of thermal regulation.
Heat production is produced by three mechanisms: voluntary muscle activity, involuntary muscle activity (shivering), non shivering thermogenisis. • Non shivering thermogenesis is the infant’s primary response to hypothermia verses shivering thermogenesis for heat production in older children and adults.
Premature or small for gestational age infants have an exceptionally large skin surface area compared with body mass and therefore loose proportionately more heat through skin than adults. • The combination of proportionally increased heat loss, and a diminished ability to produce endogenous heat, and a diminished thermoregulatory response efficacy makes infants particularly vulnerable to developing hypothermia .
Non shivering thermogenesis occurs principally through metabolism of the brown fat but can also occur at a lesser degree in the skeletal muscle, liver, brain, and white fat. Brown fat constitutes 2 to 6 % of the infant’s total body weight. • Brown fat is a highly specialized tissue with both an abundant vascular supply and a rich innervation of the sympathetic nervous system. It is activated primarily by the beta-sympathetic stimulation, this increases norepinephrin production leading to brown fat metabolism. In addition to norepinephrine , glucocorticoids and thyroxine also have been implicated in non shivering thermogenesis . • Non-shivering thermogenises can be inhibited surgically by sympathectomy and pharmaclogically by ganglionic and beta blockade, and by inhalational agents.
Thermoregulation in the newborn: • The neonate thermoregulatory range is limited and easily overwhelmed by environmental influences, the lower temperature regulation limit in the adults is 0`c, whereas in the newborn it is 22`c. • Newborns, infants, and small children are more sensitive to hypothermia because the efferent mechanisms are less effective, they have an increased surface-area-to-volume ratio, they have increased thermal conductance, and they loose proportionately more metabolic heat through the skin.
Perioperative hypothermia Mild intraoperative hypothermia is mainly due to: • Reduction in the metabolic heat production. • Increased environmental exposure. • Anesthetic induced thermoregulatory inhibition. • Redistribution of heat within the body.
General anesthesia decreases the temperature threshold at which the body initiates the thermoregulation in response to cold stress. • Hypothermia during anesthesia develops during three phases: • Internal redistribution of heat. • Thermal imbalance (heat loss to the environment). • Thermal steady state (plateau or rewarming).
Effects of anesthetic medications on thermoregulation: • General anesthesia decreases the thermoregulatory threshold temperature triggerering response to hypothermia by approximately 2.5C and increases the threshold temperature initiating responses to hyperthermia to a lesser degree. • The potent vasodilatation of isoflurane has been shown to affect the thermoregulatory threshold where its effect is inversely proportional to the inhaled concentration of isoflurane.
The influence of narcotics on thermoregulation remains controversial because their effect on animals differ than their effect on humans. Ketmine appears to cause thermoregulatory suppression than other anesthetics. • Central thermoregulation remains intact during regional anesthesia and therefore provides some protection against hypothermia. but shivering may contribute to intraoperative hypothermia.
Perioperative hyperthermia: • Similar to hypothermia which is the most thermal disturbance during anesthesia, the efferent response thresholds are displaced to the right creating a greater interthreshold range, the efferent responses during hyperthermic stress under anesthesia are limited to two mechanisms: vasodilatation and sweating. • Malignant hyperthermia is a relatively rare disorder that is estimated to occur in 1 in 50,000 to 1 in 100,000 adult patients undergoing general anesthesia, In children its incidence is reported to be 1 in 3000 to one in 15,000.
Temperature monitoring • Perioperative measurement of body temperature is necessary in infants and children to detect both hypothermia and hyperthermia. Central temperature is preferable in children to determine the severity of heat loss. ETCO2 is the earliest indicator of hypermetabolism. • Thermometers are easy and convenient to use in pediatric anesthesia and relatively inexpensive. These devices generally do not have the range or accuracy for clinical use.
Temperature monitoring sites • Temperature measurement sites may be central or peripheral, There is no physiological evidence to suggest that central temperature represents the hypothalamic temperature. • It is still suggested that the tympanic membrane is the ideal temperature monitoring site, other central sites are pulmonary artery, rectal, nasopharyngeal and esophageal temperatures, they are supposed to be similar in anesthetized children and infants undergoing non-cardiac surgery
Axillary temperature is useful only when the thermometer is carefully placed over the artery and the arm is adducted, it is as accurate as the tympanic membrane temperature, it is the most commonly used site in infants and children is the most convenient for short surgical procedures. • Nasopharyngeal temperature is measured by positioning the probe in the nasopharynx posterior to the soft palate, it should provide an estimate of the hypothalamic temperature. With the use of uncuffed endotraceal tube, this site of temperature measurement is affected by leakage of air around the endotracheal tube and may occasionally provide inaccurate readings.
Esophageal temperature probes are usually incorporated into disposable stethoscopes. It will measure central temperature reliably when the probe is placed in the lower third of the esophagus at the point where the maximum heart sounds are heard. Infants and children have minimal thermal insulation between the esophagus and the trachiobronchial tree, thus the effect of respiratory gas temperature may produce inaccurate measurements. • Rectal temperature in infants and children is similar to other central measurement sites, it may be affected by open abdominal cavity or cool blood returning from legs.
A bladder temperature is the most similar to pulmonary artery temperature, it is not useful in patients whose urine output is at or bellow normal levels. • Tympanic membrane or aural canal thermometers provide a reasonable approximation to hypothalamic temperature, recent probes no longer causes tympanic membrane perforation even with vigorous insertion, the aural canal should be blocked with cotton after probe insertion to prevent cooling of the probe with the environmental temperature. • Skin surface temperature does not correlate well with central temperature, and the difference between them doesn’t remain constant so it is better avoided.
Prevention of hypothermia • Mild postoperative hypothermia (central temperature 34-36‘c, is a common occurrence following surgery and does not impair postanesthetic recovery in infants and children undergoing surgical procedures lasting less than 3 hours. mild hypothermia may impede immune response to postoperative wound infections. • Moderate to severe hypothermia is known to cause prolonged drug effect, impaired blood coagulation and thermal discomfort, in contrast 1 to 3 degrees of central hypothermia may provide protection against global and regional ischemia, hypoxemia and malignant hyperthermia.
Preventing redistribution hypothermia • The initial reduction in core temperature (0.5-1.5s) is difficult to prevent because it result from redistribution of compartmental heat from central to peripheral compartments. it can only be prevented by preoperative warming of skin surface, so decreases redistribution.
Operating room temprtature: • Operating room temperature is the most important factor that determines heat loss during surgery, premature infants and children may require ambient temperature higher than 26 degrees to maintain normothermia.
Warming devices • Aggressive skin surface warming will cause peripheral vasodilatation and increases the temperature of the peripheral compartment so decreases redistribution of heat. Warming devices include circulating hot water warmers, infrared radiant heater and convection heaters, which circulate hot water through disposable blankets, it is the most effective. • The most important factor is the surface area covered by the blanket, in children and infants the use of head caps is useful in contrast to adults. The best convection forced air system can transfer up to 50 W across the skin surface.
Airway humification • Airway humidification in intubated patients prevents tracheal damage from dry inspired gases, increases tracheal mucus flow, and minimize respiratory heat loss. • It is much more effective in pediatric anesthesia than adult anesthesia because of higher minute ventilation per KG body weight. Humidity of 50% prevents bronchospasm and maintains normal cilia function.
Intravenous fluid warming • Heat loss due to cold intravenous fluids is clinically important when large amount of fluids are administrated rapidly. • It is better to use the fluid warmer close to the intravenous site.