Download
1 / 41
420 likes | 669 Vues
SYSTEMIC INFLAMMATION LEADING TO COMORBIDITIES ASSOCIATED WITH COPD Leonardo M. Fabbri. Comorbidities and systemic effects of COPD Cardiovascular diseases in COPD COPD in Chronic Heart Failure Cardiovascular drugs in COPD. CHRONIC DISEASE IN THE ELDERLY:

E N D
SYSTEMIC INFLAMMATION LEADING TO COMORBIDITIES ASSOCIATED WITH COPD Leonardo M. Fabbri Comorbidities and systemic effects of COPD Cardiovascular diseases in COPD COPD in Chronic Heart Failure Cardiovascular drugs in COPD
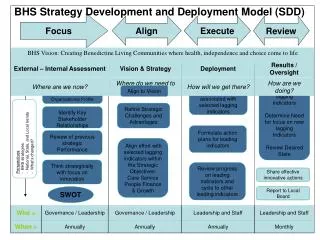
CHRONIC DISEASE IN THE ELDERLY: Back to the Future of Internal Medicine Two or more chronic diseases almost invariably develop together in the same patient, particularly in the elderly, often making it difficult to establish a proper diagnosis and assessment of severity Patient-oriented approach that takes into account the several coexisting components of chronic disease is required This “change of concept” implies the need for medical specialists to extend their expertise to broader diagnostic and treatment approaches that are traditionally the purview of internal medicine LM Fabbri and R Ferrari, Breathe, 2006, in press
Leading Causes of Death in U.S. • #1. MI • #2. CA • #3. CVA • #4. COPD Cigarette Related Diseases Leading Causes of Death Worldwide 2010
What do COPD Patients Die From? Mannino D.M., et al. Respiratory Medicine 2006; 100:115
Chronic diseases represent a huge proportion of human illness • 58 million deaths in 2005: • Cardiovascular disease 30% • Cancer 13% • chronic respiratory diseases 7% • Diabetes 2% Horton R. Lancet, 2006
COPD AS A SYSTEMIC DISEASE COPD A COMPONENT OF THE CHRONIC DISEASE • COPD A SYSTEMIC DISEASE • Systemic inflammation • Cachexia • Skeletal muscle wasting • Osteoporosis • COPD A COMORBIDITY OF • Chronic heart failure • Coronary and peripheral arterial diseases • Lung cancer • Metabolic syndrome
= ? ? ?
SYSTEMIC INFLAMMATION LEADING TO COMORBIDITIES ASSOCIATED WITH COPD Leonardo M. Fabbri Comorbidities and systemic effects of COPD Cardiovascular diseases in COPD COPD in Chronic Heart Failure Cardiovascular drugs in COPD
Cardiovascular mortality in COPD For every 10% decrease in FEV1, cardiovascular mortality increases by approximately 28% and non-fatal coronary event increases by approximately 20% in mild to moderate COPD. Anthonisen et al, Am J Respir Crit Care Med 2002
COPD CAUSES OF DEATH CAUSES OF HOSPITAL ADMISSION Curkendall et al. Ann Epidemiol 2006;16:63–70.
Prevention of Exacerbations of Chronic Obstructive Pulmonary Disease with Tiotropium, a Once-Daily Inhaled Anticholinergic Bronchodilator COEXISTING ILLNESSES Vascular (including hypertension) 64% Cardiac 38% Gastrointestinal 48% Musculoskeletal or connective tissue 46% Metabolic or nutritional 47% Reproductive or urinary 27% Neurologic 22% Niewoehner,et al, Ann Intern Med. 2005;143:317-326
Coronary Artery Calcification in Older Adults Newman AB et al Circulation 2001
Occurrence and Prognostic Significance of Ventricular Arrhythmia Is Related to Pulmonary Function 402 men, 68 yrs old – 14 yrs follow-up Engstrom G et al Circulation 2001
Carotid Plaque, Intima Media Thickness, Cardiovascular Risk Factors, and Prevalent Cardiovascular Disease in Men and Women 800 soggetti, età media 66 anni 65.4 % 59.2% 50.4% 50% Percentuale di soggetti (maschi) con una placca carotidea FEV1 terzilies Ebrahim S et al Stroke 1999
RR per maschi RR per femmine FEV1 e risk of stroke:the Copenhagen Stroke Study 4 RR per maschi e femmine 2 Rischio Relativo 1.5 1 0.5 ≥100% 90-99% 80-89% 70-79% 60-69% 50-59% <50% Percentuale FEV1 rispetto al previsto Truelsen T et al Int J Epidemiol 2001
PULMONARY EMBOLISM IN PATIENTS WITH UNEXPLAINED EXACERBATION OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE: PREVALENCE AND RISK FACTORS 25% pulmonary embolism in patients with COPD hospitalized for severe exacerbation of unknown origin Previous TEP, malignancy, low PaCO2 Tillie-Leblond et al, Ann Intern Med. 2006;144:390-396.
Cardiovascular morbidity in COPD P=0,001 Cardiac infarction injury score High CRP and severe obstruction High CRP Severe obstruction Sin and Man, Circulation 2003
Inflammation, atherosclerosis and coronary artery disease Hansson GK, N Engl J Med. 2005;352(16):1685-95 Activation of a type 1 immune response in atheroma formation
Cross-sectional study, patients 65 years of age • Of 405 participating patients with a diagnosis of chronic obstructive pulmonary disease, 83 (20.5%, 95% CI 16.7–24.8) had previously unrecognized heart failure
RECOGNISING HEART FAILURE IN ELDERLY PATIENTS WITH STABLE CHRONIC OBSTRUCTIVE PULMONARY DISEASE IN PRIMARY CARE A limited number of items easily available from history and physical examination,with addition of NT-proBNP and electrocardiography, can help general practitioners to identify concomitant heart failure in individual patients with stable COPD F H Rutten et al, BMJ 2005, Dec;331(4):1379-81
Peptidi natriuretici ANP Peptide natriuretico atriale BNP Peptide natriuretico cerebrale ANP ANP BNP BNP Cuore normale Cuore scompensato Peptidi natriuretici come marker dello scompenso cardiaco cronico
Breathing Not Properly Multinational Study • 1586 participants who presented with acute dyspnea • 1538 (97%) had clinical certainty of CHF determined by the attending physician in the emergency department • Participants underwent routine care and had BNP measured in a blinded fashion • ~ 37 % COPD comorbidity McCullough et al. Circ 2002
Breathing Not Properly (BNP) Multinational Study McCullough et al. Circ 2002
Utility of BNP in Differentiating Heart Failure from Lung Disease in Patients Presenting with Dyspnea Morrison et al. JACC 2002
Utility of BNP in Differentiating Heart Failure from Lung Disease in Patients Presenting with Dyspnea Morrison et al. JACC 2002
SYSTEMIC INFLAMMATION LEADING TO COMORBIDITIES ASSOCIATED WITH COPD Leonardo M. Fabbri Comorbidities and systemic effects of COPD Cardiovascular diseases in COPD COPD in Chronic Heart Failure Cardiovascular drugs in COPD
Acute MI(0.5–10 days)—SAVE, AIRE or TRACE eligible(either clinical/radiologic signs of HF or LV systolic dysfunction) Major Exclusion Criteria: — BP < 100 mm Hg — Serum creatinine > 2.5 mg/dL — Prior intolerance of an ARB or ACEI — Nonconsent double-blind active-controlled Captopril 50 mg tid (n = 4909) Valsartan 160 mg bid (n = 4909) Captopril 50 mg tid + Valsartan 80 mg bid (n = 4885) median duration: 24.7 monthsevent-driven Primary Endpoint: All-Cause Mortality Secondary Endpoints: CV Death, MI, or HF Other Endpoints: Safety and Tolerability
VALIANT Trial:Prevalence of COPD • 14703 patients included in the trial • 1258 clinical diagnosis of COPD (8.6%)
Study Design HF patients 18 yr; NYHA II–IV LVIDD> 2.9 cm/m² BSA; EF<40% Receiving Standard Therapyincluding ACE inhibitors , diuretics digoxin , -blockers Randomized to Valsartan40 mg bid titrated to160 mg bid Placebo 906 deaths (events reported) J. N. Cohn et. al, J. Card. Fail. 1999; 5: 155-160
Val-HeFT Trial:Prevalence of COPD • 5010 patients included in the trial • 628 clinical disgnosis of COPD (12.5%)
Val-HeFT TrialClinical events at 2 year follow-up Mortality Hospitalization <0.0001 P value <0.0001
Contributors to exercise intolerance in COPD and CHF Gosker et al. AJCN 1999
SYSTEMIC INFLAMMATION LEADING TO COMORBIDITIES ASSOCIATED WITH COPD Leonardo M. Fabbri Comorbidities and systemic effects of COPD Cardiovascular diseases in COPD COPD in Chronic Heart Failure Cardiovascular drugs in COPD
METHODS • Case-control study of two population-based retrospective cohorts • COPD patients having undergone coronary revascularization (high CV risk cohort) • COPD patients without previous myocardial infarction (MI) and newly treated with nonsteroidal anti-inflammatory drugs (low CV risk cohort) • Outcomes: COPD hospitalization, MI, and total mortality Mancini GB, et al. J Am Coll Cardiol. 2006 Jun 20;47(12):2554-60
REDUCTION OF MORBIDITY AND MORTALITY BY STATINS, ANGIOTENSIN-CONVERTING ENZYME INHIBITORS, AND ANGIOTENSIN RECEPTOR BLOCKERS IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE These drugs reduced both CV and pulmonary outcomes Largest benefits with statins combined with ACEin or ARBs This combination reduces COPD hospitalization and mortality in the high and low CV risk cohort The combination also reduced MI in the high CV risk cohort Benefits were similar when steroid users were included Mancini GB, et al. J Am Coll Cardiol. 2006 Jun 20;47(12):2554-60
REDUCTION OF MORBIDITY AND MORTALITY BY STATINS, ANGIOTENSIN-CONVERTING ENZYME INHIBITORS, AND ANGIOTENSIN RECEPTOR BLOCKERS IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE These agents may have dual cardiopulmonary protective properties, thereby substantially altering prognosis of patients with COPD These findings need confirmation in randomized clinical trials Mancini GB, et al. J Am Coll Cardiol. 2006 Jun 20;47(12):2554-60
SYSTEMIC INFLAMMATION LEADING TO COMORBIDITIES ASSOCIATED WITH COPD Leonardo M. Fabbri Comorbidities and systemic effects of COPD Cardiovascular diseases in COPD COPD in Chronic Heart Failure Cardiovascular drugs in COPD