Download
1 / 35
1.31k likes | 9.54k Vues
TREATMENT OF ANAL FISSURES. ANAL FISSURE - DEFINITION. “ A crack or a tear in the vertical axis of the squamous lining of the anal canal between the anal verge and the dentate line “. Sentinel Skin Tag. Fissure. Anal Polyp. ACUTE FISSURE

E N D
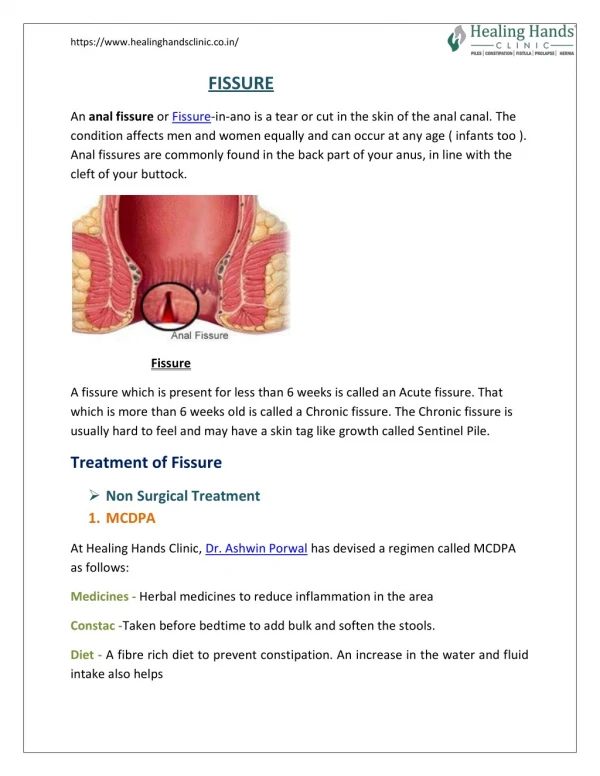
ANAL FISSURE - DEFINITION “A crack or a tear in the vertical axis of the squamous lining of the anal canal between the anal verge and the dentate line “ Sentinel Skin Tag Fissure Anal Polyp
ACUTE FISSURE Painful cleft in the anoderm exposing submucosa and possibly the internal sphincter CHRONIC FISSURE Anodermal cleft with scarred base and surrounding inflammation. Frequentlly seen with hypetrophied anal papilla and “sentinel pile” ANAL FISSURE - CLASSIFICATION
CHRONIC FISSURE Deep indurated anal ulcer Elevated, overhanging edges Associated scarring “Sentinel pile”+hypertrophied papilla Visibile sphincter fibers Rarely lateral Less pain at defecationwith gradually decreasing intensity (lasts from minutes to several hours). No nocturnal Pruritus Blood on occasion ACUTE FISSURE Superficial without fibrosis Flat edges None (unless prior surgery) None Not always visible May be lateral Severe, sudden stinging sharp pain associated with defecation (lasts only a few minutes) No pruritus Blood usual, bright red, stains paper or drips into the toilet ANAL FISSURE - PRESENTATION
ANAL FISSURE - ETIOLOGY • Associated with passage of hard stool • Associated with sphincteric hypertone • ? Most common in posterior midline • ? Some heal spontaneously vs. become chronic
ANAL FISSURE - PATHOGENESIS • Abnormality of internal sphincter • High resting pressures • NO: Duthie & Bennet, 1964; Braun, Raguse & Dohrenbusch, 1986 • YES: Northmann & Schuster, 1974; Hancock, 1977; Abcarian, 1982 • DIGITAL EXAMINATION IS UNRELIABLE: Jones OM, Ramaligam T, Lindsey I, et al. Dis Colon Rectum 2005, 48:349-352 • Abnormal reflex relaxation in response to rectal distention • Ischemia • Posterior commissure is less perfused • Klosterhalfen B, Vogel P, Rixen H, et al. Dis Colon Rectum 1989; 32:43-52 • Schouten WR, Briel JW, Aurweda JJA. Dis Colon Rectum 1994; 37:664-9
Intersphincteric abscess Pruritus ani Crohn’s disease Ulcerative Colitis Tuberculous anal fissures Syphilitic anal fissures AIDS Leukemia Anal Malignancy Previous surgery (hemorroidectomy, fistula-in-ano) Childbirth ANAL FISSURE - DIFFERENTIAL DIAGNOSIS
Men=Women Posterior fissure most common Anterior fissure most common inwomen (10%) Both anterior and posterior (10%)
ANAL FISSURE - TREATMENT ACUTE FISSURE MEDICAL TREATMENT CHRONIC FISSURE SURGICAL TREATMENT
CONSERVATIVE MEDICAL TREATMENT • Correct precipitating cause (constipation, diarrhea) • Increased fluid • Sitz baths, bran, bulk laxatives • Topical Steroids • Local anesthetics • (solcoderm, sodium tetradecyulfate, anal dilators) Effective in up to 50% of cases (placebo in up to 35% of cases)
ANAL FISSURE - CONSERVATIVE TREATMENT N = 103 patients Jensen SL. BMJ 1986; 292:1167-1169
ANAL FISSURE - NEW MEDICAL TREATMENTS • NO Donors • Glycerin trinitrate-GTN; Isosorbide dinitrate-ISDN • Calcium Channel Blockers • Nifedipine, Diltiazem • Botulinum Toxin • Gonyautoxin Reduce MRP - Increase microcirculation
MEDICAL TREATMENT - NO DONORS(Glycerin trinitrate - Isosorbide dinitrate) • Significant decrease in MRP • Effective at concentration from 0, 2% to 0, 5% • Immediate relief of pain that lasts for 2-6 hours • Healing 30% in 4-6 weeks, 86% in 3 months • Need for frequent application • Headache between 20 to 84% (commonly around 25%) • Discontinuation of therapy up to 20% • Recurrence rate up to 30%
MEDICAL TREATMENT CALCIUM CHANNEL BLOCKERS • Significant decrease in MRP • Healing from 65% to 95% • Side effects: headache (up to 25%), flushing, hypotension • Oral administration: lower healing rate, higher complications • Recurrence rate: up to 42 %
MEDICAL TREATMENT - BOTULIN TOXIN • Since 1993 • Significant decrease in MRP (30%) • Two doses of 0,1 ml diluted toxin • Healing from 43% to 96% • Chemical denervation lasts 2 to 3 months • Transient incontinence: flatus 10-12%, stool 5% • Recurrence rate around 20% • Expensive
MEDICAL TREATMENT - GONYAUTOXIN • Phytotoxin produced by microscopic planctonic algae • Stored in filter feeders like bivalves • Blocks the voltage-gated sodium channels in a reversible way • Two doses of 100 units (second one after 7 days) • Reduces both and MRP and MVCP • Immediate post injection sphincter relaxation and relief of pain • Healing rate: 98% in 28 days • Recurrence rate: ??? • Further studies needed Garrido R, Lagos N, Lattes K et al. Gonyautoxin: new treatmentfor healing acute and chronic anal fissures. Dis Colon Rectum 2005, 48:335-343
ANAL FISSURE - SURGICAL TREATMENT HISTORY 1838 Recamier - Anal stretch 1835 Brodie 1892 Goodsall 1930 Gabriel 1934 Milligan & Morgan 1939 Miles - “pectenotomy” (division of “pecten band”) • Eisenhammer - open lateral internal sphincterotomy • Notaras - closed lateral subcutaneous internal sphincterotomy sphincterotomy fissurectomy
ANAL FISSURE - SURGICAL TREATMENT • Anal Dilatation • Fissurectomy and Posterior Sphincterotomy • Open Lateral Internal Sphincterotomy • Closed lateral Internal Sphincterotomy • Anoplasty (advancement flap, V-Y flap, rotational flap, etc.)
ANAL DILATATION • Still popular in the UK (36% of surgeons) • Sphincter damage in > 50% of patients • Incontinence to flatus 12,5 - 28.6% • Major incontinence 2 - 7,1% • Soiling up to 39.3% • 4 fingers x 4 minutes • Parks retractor at 4.8 cm • Healing rates from 43/ to 94% • Recurrence rate:10 to 30%
FISSURECTOMY-POSTERIOR SPHINCTEROTOMY • Cure rate : 93% • “Keyhole” deformity: 5% • Incontinence to flatus: 17-34% • Incontinence to feces: 3 -15% • Soiling up to 41% • Large external wound • Prolonged time for healing • Recurrence rate: 1,3 % Gabriel WB , 1930
LATERAL INTERNAL SPHINCTEROTOMY OPEN - Eisenhammer S, 1951 CLOSED - Notaras MJ, 1969
LATERAL INTERNAL SPHINCTEROTOMY No difference for persistence of symptoms, fissure recurrence or need for reoperation between open and close. Statistical significant difference for soiling of underwear (26,7% vs. 16,1%) and stool incontinence (11,8% vs. 3,1%). Almost significant for flatus incontinence (30,3% vs. 23,6%). Garcia-Aguilar et al., 1996 No difference between the two methods. Nelson RL, 1999 Boulous PB et al., 1984 Kortbeek JB et al., 1992
ANAL FISSURE - TREATMENT “…Fully 45% of patients had some degree of fecal incontinence at some point after LIS. However, by one month after surgery, only 6% were incontinent to flatus. More importantly, 98% of patients were satisfied with the outcome of surgery, and < 1% of patients had their life affected by incontinence…” Nyam DC, Pemberton JH, Dis Colon Rectum1999; 42:1306-10
LATERAL INTERNAL SPHINCTEROTOMY • Forceful anal dilatation is inferior to LIS owing to a higher recurrence rate with higher rates of incontinence Olsen J et al., 1987 Weaver RM et al., 1987 • LIS is superior to fissurectomy and posterior midline sphincterotomy owing to faster healing rates, less pain and less postoperative incontinence Abcarian H, 1980 Saad AM et al., 1992 • LIS is superior to anal dilatation and posterior midline sphincterotomy Nelson R, 2004
ANOPLASTY Advancement Flap V-Y Flap Rotational Flap
ANOPLASTY • Associated stenosis (mild, moderate, severe) • Usually postoperative (hemorrhoidectomy, fistulotomy) • In patients with normal or low MRP • In recurrences • V-Y flaps: 60-70% of donor sites break down and median healing time of 4 months (2 - 6) • Rotational flap: lower break down rate • No incontinence • A viable alternative to LIS Leong AF, Seow-Choen F. Dis Colon Rectum 1995;38:69-71 Kenefick NJ, Gee AS, Durdey P. Colorectal Dis 2002; 4:463 Singh M et al. Int J Colorectal Dis 2005; 20:339-42
ANAL FISSURE PERSONAL SURVEY (1993-2004) 295 Pts Male:151 Female: 144 Mean FU: 96 mths (18-150) Post.: 255 (87,5%) Ant.: 40 (13%) Both: 31(10%) 274 (93%) operated on under local anesthesia Open LIS: 239 (81%) Post. IS+Fissurectomy 5 (1,6%) Advancement flap 27 (9%) V-Y flap 23 (8%) Rotation Anoplasty 1 (0, 4%) Associated Excision 146 (50%) Associated pathologies 211 (70%) (hemorrhoids 62%; mucosal prolapse 19%; hemorrhoids+mucosal prolapse 11%; fistula-in-ano 1%)
ANAL FISSURE PERSONAL SURVEY (1993-2004) LIS Incont. Flatus: 21 (8,7%) Soiling: 11 (4,5%) Recurrence: 2 (0,6%) Hematoma: 8 (3%); Perianal abscess: 1 (0,4%) ; Thrombosed Hemorrhoids: 1 (0,4%) ; Hemorrage: 2 (0,8%) Post. IS 1/5 not healed at 3 months (DTC); 1/5 Incont. Flatus+Soiling Advancement Flap 6/27(22%) Ant.+Post. - 3/27 (11%) Breakdown - Healing T: 7,7 wks (2-40) V-Y Flap 1 deceased - 15/22 (68%) Breakdown - Healing T: 6,5 wks (3-12)
ANAL FISSURE-COMPARISON OF TREATMENT Nelson R. Dis Colon Rectum 2004, 47 (4):422-431
ANAL FISSURE - TREATMENT “…first line use of medical therapy cures most chronic anal fissures cheaply and conveniently…” Lindsey I, Jones OM, Cunningham C, Mortensen NJ. Br. J. Surg 2004;91:279-9 “…medical therapy for chronic anal fissure may be applied with a chance of cure that is only marginally better than placebo… [and] far less effective than surgery…” Nelson R. Dis Colon Rectum 2004;47:422-31
ASCRS PRACTICE PARAMETERS • Conservative therapy is safe, has few side effects, and should usually be the first step • Anal fissures may be appropriately treated with topical nitrates because they can relieve pain; however, nitrates are only marginally associated with a healing rate superior to the placebo • Anal fissures may be appropriately treated with topical calcium channel blockers, which seem to have a lower incidence of adverse effects than nitrates. There is insufficient data to conclude whether they are superior to placebo in healing fissures • Botulinum toxin injections may be used for anal fissures that fail to respond to conservative measures and have been associated with a healing rate superior to placebo. There is inadequate consensus on dosage, precise site of administration, number of injections or efficacy
ASCRS PRACTICE PARAMETERS • Lateral internal sphincterotomy is the surgical treatment of choice for refractory anal fissures • Open and closed technique for LIS seem to yield similar results • Anal advancement flap is an alternative to LIS; further study is required • Surgery may be appropriately offered without a trial of pharmacologic treatment after failure of conservative therapy; patients should be informed about the potential complications of surgery
THANK YOU FOR YOUR ATTENTION! “The one who knows much talks little. The one who talks much does not know” Lao Tse