Download
1 / 45
450 likes | 658 Vues
The combination of low dose of naloxone and morphine in PCA. 10/4 Morning Meeting Yu Chang Yeh. The combination of low dose of naloxone and morphine in PCA. Objective Backgrounds Patient selection and exclusion Standard setup. The combination of low dose of naloxone and morphine in PCA.

E N D
The combination of low dose of naloxone and morphine in PCA 10/4 Morning Meeting Yu Chang Yeh
The combination of low dose of naloxone and morphine in PCA • Objective • Backgrounds • Patient selection and exclusion • Standard setup
The combination of low dose of naloxone and morphine in PCA • Intolerable side effects • Low side effects setup • Treatment failure and withdrawal • Relevant studies
Objective • Dose the combination of low does naloxone and morphine in PCA reduce the incidence of side effects and requirement of morphine?
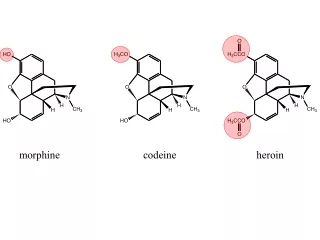
Backgrounds 1 • Without antiemetic drugs, the incidence of nausea was on average 43%, of vomiting was 55%, and of any emetic event was 67%.(1) • Tramer MR, Walder B. Efficacy and adverse effects of prophylactic antiemetics during patient-controlled analgesia therapy: a quantitative systematic review. Anesth Analg 1999;88:1354-61
Backgrounds 2 • Pruritus 55% • Gan TJ, Ginsberg B, Glass PS, Fortney J, Jhaveri R, Perno R. Opioid-sparing effects of a low-dose infusion of naloxone in patient-administered morphine sulfate. Anesthesiology 1997;81:77-84
Backgrounds 3 • Low dose naloxone infusion (0.25ug/kg/hr) was effective in reducing the incidence of nausea, vomiting, and pruritus. It also deceased opioid requirements. • Placebo/ 0.25ug/kg/hr/ 1ug/kg/hr • 20/20/20 --- total 60 • Gan Anesthesiology 1997;81:77-84
Backgrounds 4 • 1ug/kg/hr decreases opioid-related side effects but seemed to attenuate the pain relief provided by morphine. 64.7+/- 33mg vs 59.1 +/- 27.4mg in Placebo • Gan Anesthesiology 1997;81:77-84 • Included in Miller Anesthesia
Backgrounds 5 • In animal study • Enhanced release of endogenous opiates • Up-regulation phenomenon • Within 30 min • Paronis CA J Pharmaol Exp Ther 1991;259:582-9. • Yoburn BC J Pharmaol Exp Ther 1986;239: 132-5.
Backgrounds 6 But…… • Direct combination of naloxone and morphine in PCA does not decrease opioid requirements or morphine-related side effects in the postoperative period. • Cepeda MS, Africano JM, Manrique AM, Fragoso W, Carr DB. Pain 2002;96:73-79
Backgrounds 7 • Systemic reviews suggest that prophylaxis does not work very well, that there is a finite risk of adverse drug reactions with most antiemetic intervention, ant the treatment may be more cost effective than prophylaxis. • Tramer MR. A rational approach to the control of postoperative nausea and vomiting: Acta Anesth Scand 2001;45:14-19
Backgrounds 8 • We try to find out an optimal combination ratio of naloxone and morphine in PCA to reduce the severity of side effects related with PCA morphine. • Only patients suffered form intolerable side effects were enrolled in our study.
Patients selection Inclusion criteria 1. Age 18-65y/o 2. ASA I-III 3. Surgical procedure < 5 hrs 4. Use PCA for postoperative pain control 5. Who suffers form intolerable side effects
Patient exclusion 1. Intraoperative Fentanyl use 4μg/kg 2. Patient with hiatal hernia and esophageal reflux symptoms 3. Recent use of antiemetics or antipruritic treatment after 4. Recent use of NSAIDs after operation
Standard PCA Setup • Morphine 1mg/ml • PCA dose 2ml • Lockout time 10min • No continuous dose
Intolerable side effects • Nausea and vomiting • Pruritus • Urinary retention • Change in consciousness • Respiratory depression
Low side effect PCA setup • PCA • Morphine 1mg/ml • Naloxone 2μg/ml • PCA dose 2ml • Lockout time 10min • No continuous dose
Treatment failure • Nausea and vomiting • Pruritus • Urinary retention • Change in consciousness • Respiratory depression • Increase intensity of pain
Withdrawal • Withdrawal • Adjunct drugs for side effects
Measurements and Evaluation • Evaluation of Pain intensity • Pain on exertion – verbal numerical scale 0-10 • Pain at rest – verbal numerical scale 0-10
Measurements and Evaluation • Evaluation of side effects • Nausea – • 0 absent • 1 mild • 2 moderate • 3 severe • Vomiting – • number of events
Measurements and Evaluation • Pruritus – • 0 absent • 1 mild • 2 moderate • 3 severe • Urinary retention – • yes / no
Measurements and Evaluation • Consciousness – • 0 alert • 1 sleepy • 2 stupor • 3 coma • Respiratory depression – • respiratory rate
Relevant Studies 1 • Naloxone – other applications 1 • Septic and hemorrhagic shock • Alcoholism • Poatanesthetic apnea in infants • Primary apnea and periodic breathing associated with hypoxemia • Restore flow-resistive load compensation in patients with COPD
Relevant Studies 2 • Naloxone – other applications 2 • May ameliorate the neurologic deficit following an ischemic or traumatic neurologic insults in animals
Relevant Studies 3 • Other Opioid antagonist • Naltrexone • Nalmefene • Long acting • Equipotent to naloxone • Plasma half life 3-10hours • Naloxone 64 +/- 12min • Morphine 2-7hours
Relevant Studies 4 • Effects of prophylactic nalmefene on the incidence of morphine-related side effects in patients receiving intravenous PCA • Saline/ 15ug nalmefene / 25ug nalmefene • Decrease the need for antiemetics and antipruritic medications
Relevant Studies 5 • Lidocaine+Morphine vs Morphine alone • Music • Men and women • Naloxone vs PCEA
Relevant Studies 6 • 1999 systemic review • Droperidol • Clonidine • Ondansetron • Tropisetron • Metoclopramide • Hyoscine • Promethazine
Relevant Studies 7 • 2000 British Journal of Anesthesia • Prevention of postoperative nausea and vomiting by continuous infusion of subhypnotic propofol in female patients receiving intravenous PCA • Placebo, 5, 10, 15, 20 ug/kg/min • No symptoms 25%,40%,45%,65%,75%
Relevant Studies 8 • Total fentanyl consumption • Placebo, 5, 10, 15, 20 ug/kg/min • 413/585/537/514/712 ug
Thanks for your attention! Have a nice day!
Sample size • Null hypothese / one or two sided alternative hypothese • Appropriate statistical test • Choose a reasonable effect size (and variability if necessary) • Set α,β • Use the appropriate tables or formula
E/S • Effect Size (E) • The difference in the mean value of the outcome variable between the study group • Standard deviation(S) • The variability of the outcome variables • Standard effective size (E/S) • For most study 0.1-0.5
Example • The efficacy of Salbutamol and ipratropium bromide for the treatment of asthma • FEV1 after 1 week treatment • Previous study Mean 2liter with S 1liter • Effective size 0.2liter (10%) • Standard effective size 0.2/1 = 0.2
Example • α= 0.05 • β= 0.2 (power = 0.8) • Look across the Table • 394 for each group
Example • Sample size (per equal-sized group) • = 16 / (E/S)2 • Try to reduce the sample size • Increase E • Decrease S