Download
1 / 25
270 likes | 404 Vues
Sleep Disturbances in Parkinson’s. Angela Anagnos, MD Board Certified in Sleep Medicine and Neurology www.sleepmedicineandneurology.com. Introduction most people with PD find it difficult to sleep through the night. Rigid muscles Tremors or stiffness Unable to roll over in bed

E N D
Sleep Disturbances in Parkinson’s Angela Anagnos, MD Board Certified in Sleep Medicine and Neurology www.sleepmedicineandneurology.com
Introduction most people with PD find it difficult to sleep through the night • Rigid muscles • Tremors or stiffness • Unable to roll over in bed • Frequent urge to urinate • Vivid dreams, hallucinations, violent nightmares • Acting out dreams(RBD) can precede PD by decades
Daytime Sleepiness • Due to sleep disturbances • Due to medication side effects • Due to Parkinson’s disease itself • End result: Interferes with daily life
Step 1: Find Root Cause • Seek professional help in early or mid-stage PD for: • Insomnia • Excessive daytime sleepiness • Restless legs syndrome • REM behavior disorder • Poor sleep due to depression
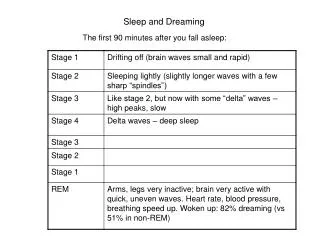
Insomnia • Inability to get a good night’s sleep • Trouble falling/staying/falling back to sleep • Fragments of sleep a few hours at a time • Sleep studies (PSG) in PD show: • Less deep sleep (S3) • More light sleep (S1S2) • Increased sleep fragmentation • Multiple night awakenings
Sleep Hygiene and Insomnia • Maintain a regular schedule for waking/sleeping • Avoid excessive time in bed • Avoid naps during the day and early evening • Use bed for sleeping (not reading or watching TV) • Do not watch the clock in bed • Try to relax before bedtime: environmental cues • Timed light exposure in the am
Sleep Hygiene • Keep the bedroom dark, cool and comfortable • Block out noises that disturb sleep • Avoid caffeinated beverages or alcohol w/in 6 hrs of bedtime • Exercise early in the day, not two hours before bedtime • Go to another room if you cannot sleep • Avoid going to bed hungry
Light Therapy • Do not underestimate the power of natural sunlight in helping circadian rhythm disorders and common insomnia!
Excessive Daytime Sleepiness in PD • Common in early and mid-PD • Can be related to insomnia • Can be related to other sleep disturbances • Sleep apnea • RLS/PLMD • RBD • Or related to medications • High doses of dopaminergic medications like pramipexole and ropinirole can contribute but rare
RLS- Restless Legs Syndrome • 5-10% of general population • Common in PD but not predictive of PD • Can predate PD by many years/decades • Common, underdiagnosed, hyperkinetic movement disorder
RLS • Four diagnostic criteria • Do you have an uncomfortable or unpleasant sensation that causes an urge to move your legs? • Are your symptoms worse during periods of rest or inactivity such as lying or sitting? • Are your symptoms temporarily relieved by movement, such as walking or stretching? • Are your symptoms worse in the evening or at night? As symptoms get worse, can occur during the day • Key ?: “Do you have a creepy, crawly, or restless feeling in your legs at night that improves when you move around?”
RLS • Usually primary/hereditary (possible loci chromosomes 9,12,14) • Secondary causes due to iron deficiency, ESRD, Medications (neuroleptics=DA antagonists like Reglan) or antidepressants, peripheral neuropathy • Prevalence increases with age over 40, F>M • Can be mistaken for ADHD, especially in children • More common in Parkinson’s Disease
PLMS-Periodic Limb Movements in Sleep • 80% of those with RLS also have PLMS • Slow, involuntary, stereotypic movements, usually involving flexing the leg at the hip, knee, and ankle. May involve arms. • Reported by bed partner or found on sleep study. • Causes daytime sleepiness and/or insomnia
RLS/PLMD Work-Up • Labs tests for blood count, ferritin and iron studies, folate, glucose, renal screen; EMG/NCV if suspect neuropathy • Sleep study to rule out sleep apnea and look for PLMD
TREATMENT RLS/PLMD • Avoid alcohol, caffeine; regular sleep hygiene • Stop problematic medications like antihistamines, tricyclic antidepressants • Dopamine agonists help >70% of patients ; first line therapy : ropinirole (Requip) pramipexole (Mirapex), Levodopa (Sinemet) • anticonvulsants like gabapentin, carbamazepine • narcotics, iron tid with Vit C if ferritin < 50 mcg/dL or iron saturation <16%
REM Behavior Disorder (RBD) • A disorder of dissociation of muscle atonia during REM sleep • Breakthrough behaviors during REM described as acting out dreams • Abrupt emotional vocalizations, swearing, injurious/violent behaviors • Disruption of sleep continuity • Appx 50% of PD patients have partial or complete loss of muscle atonia in REM sleep
REM Behavior Disorder (RBD) • Male predominance > 45 yrs • Associated neurodegenerative diseases, PD • Morbidity • Self injury 1/3 of cases • Injury to others 2/3 of cases • Daytime sleepiness in ¾ of cases (often due to other associated sleep problems)
Treatment of RBD • Behavioral • Safe environment • Reduce disruptive events • Reduce anxiety • Good sleep hygiene • Pharmacological • Clonazepam (80% of patients reported benefit) • Parkinson’s Treatment with Dopaminergics
Obstructive Sleep Apnea (OSAS)Symptoms • Snoring • Witnessed apneas • Daytime fatigue/Sleepiness • Moodiness, irritability • Concentration/ memory complaints • Depression • Insomnia • Exacerbated pain symptoms
Whose at Risk? • Men> premenopausal women • Micrognathia, overbite • Obesity, hypothyroidism • Enlarged adenoids, tonsillar tissue • Exacerbated by supine sleep, gravity • Deviated septum, allergies with mouth breathing • Macroglossia, enlarged uvula • Decreased muscle tone with aging, testosterone • Higher incidence in PD related autonomic dysfunction
Diagnosis of OSAS by PSG • Apneas- cessation of airflow >10 sec • Hypopneas- 50% reduction in airflow with 3% reduction in oxygen, or EEG arousal • RERAS- EEG arousals with increased respiratory effort • AHI> 5/hr • RDI > 40/hr, severe
Treatment of OSAS • CPAP/BIPAP/ AutoPAP +/- oxygen • Weight loss • Mandibular Advancement Appliance • Surgery overall, 50-70% improvement • UPPP • Septoplasty, turbinate reduction • Maxillomandibularadvacement • Somnoplasty (RF) • Pillar procedure • tracheostomy
Sleep and Depression • Depression in appx 40% of PD patients • Associated with sleep disturbances • Unrefreshing sleep • Early morning awakenings • Irregular dreams
Sleep in Later Stages of PD • 33% of PD patients in mid-late stages experience hallucinations related to higher doses of medications • Visual, not auditory • Associated with vivid dreams