Download

1 / 58
580 likes | 726 Vues
Causes of missing mammographic lesions. Dense parenchyma that obscures a lesion Poor positioning or technique Lesion location outside the field of view Lack of perception of an abnormality that is present Incorrect interpretation of a suspect finding Subtle features of malignancy

E N D
Causes of missing mammographic lesions • Dense parenchyma that obscures a lesion • Poor positioning or technique • Lesion location outside the field of view • Lack of perception of an abnormality that is present • Incorrect interpretation of a suspect finding • Subtle features of malignancy • A slowly changing malignancy
. Breast cancers are easily missed when they appear as focal areas of asymmetry or distortion (eg, invasive lobular carcinoma) • when their appearance suggests a benign cause (eg, medullary and mucinous [colloid] invasive ductal carcinomas, which usually manifest as mostly circumscribed masses). • Bird et al (6) found that 77 of 320 cancers (24%) in a screening population were missed, primarily due to dense breasts and a developing density that was not identified by the radiologist • Goergen et al (7) found that cancers missed at screening mammography were significantly lower in density and were more often seen on only one of two views than were detected cancers
Any patient with dense breast parenchyma, a palpable mass, and negative mammographic findings should undergo US for further evaluation of the mass.
The negative predictive value of US with mammography for a palpable lesion to be 99.8% and 100%, respectively. Moy et al (11) found the negative predictive value of US with mammography for a palpable mass to be 97.4%. However, a palpable mass that appears solid at US warrants further evaluation with biopsy.
craniocaudal RL = “craniocaudal rolled laterally”). craniocaudal RL = “craniocaudal rolled laterally”).
Radiologists’ Errors • Lack of Perception • Satisfaction of search • Error of Interpretation • Do not compare with Previous study
Conclusion • Although mammography is the standard of reference for the detection of early breast cancer, as many as 30% of breast cancers may be missed. To reduce the possibility of missing a cancer, the radiologist should take the following steps when interpreting mammographic findings: • Do not rely on screening views alone to diagnose a detected abnormality; complete the evaluation with diagnostic mammography. • Review clinical data and use US to help assess a palpable or mammographically detected mass. • Be strict about positioning and technical requirements to optimize image quality. • Be alert to subtle features of breast cancers. • Compare current images with multiple prior studies to look for subtle increases in lesion size. • Look for other lesions when one abnormality is seen. • Judge a lesion by its most malignant features.
Reporting Mammogram Using BIRADS • Brief description of reason for the MMG • Brief description of the type • Comparison with previous MMG • Description of finding • Final assessment categories • Recommendation
BIRADS0, Recommendations • Dense Breast in screening ,young high risk: MRI • Dense Breast & Palpable Mass: US, Solid, complex cyst: CNB, Thick- wall cyst: Aspiration • Mass without fat or characteristic MicCal: US, Solid, <5mm suspicious: VAB, circumscribed: local Mag view • Absence of previous exam • Indeterminate findings: Additional views
BIRADS 1, negative for malignancy • Normal fatty breast: Routine FU • Negative symmetrical SFG, No change or neodensity: FU • Heterogeneously symmetrical dense, no pertinent finding, no change or neodensity, may recommend US
BIRADS2, Benign finding • An intra mammary lymph node • Benign miccals • Fat contained masses • Thin -wall cysts with or without Int echo
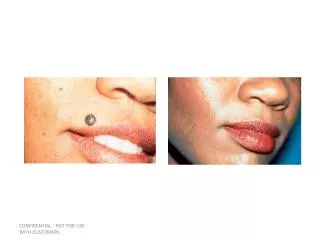
Tangential spot magnification mammogram, obtained after placement of an external marker,BIRADS2 Oil cyst
BIRADS3, Probably benign,<%2 malignancy, Short term FU • An oval shape, well- defined, circumscribed or macro lobulated mass which is solid, isoechoic, and parallel on US: 6, 12, 24 moths FU, increased size of %25 : CNB • Monomorph cluster Miccal: 6,12, 24 months FU • Focal asymmetry+ nonpalpable+ negative US
BIRADS4a, 3-30% malignancy, VAB or CNB • Probably benign appearance with a tail or mild inhomogeneity on US • Probably benign but hypo echoic mass • Intra cystic mass, intra ductal papilloma :VAB • Thick wall cyst : Aspiration • Indeterminate Amorphus cluster Miccal: VAB • Developing density • Focal asymmetry+ palpable lump+ Neg US
Type 2 complex cyst+ doppler,BIRADS4a, CNB Papillary apocrine hyperplasia with atypical ductal hyperplasia
Infiltrating Ductal Ca Complex cyst, irregular thick wall
BIRADS4b 30- 60% malignancy, VAB or CNB • Round circumscribed masses • Round hypo echoic masses • Structural distortion without history of surgery or infection: VAB • New asymmetry: VAB