Download
1 / 1
10 likes | 91 Vues
Projected line. Relaxed hand position. Cause. Initial response. Secondary response and outcome. Reorganisation of motor control strategies. Superficial tissue damage Initial pain. Alteration of superficial dynamic muscle activation (pain adaptation). Repetitive non-impact injury

E N D
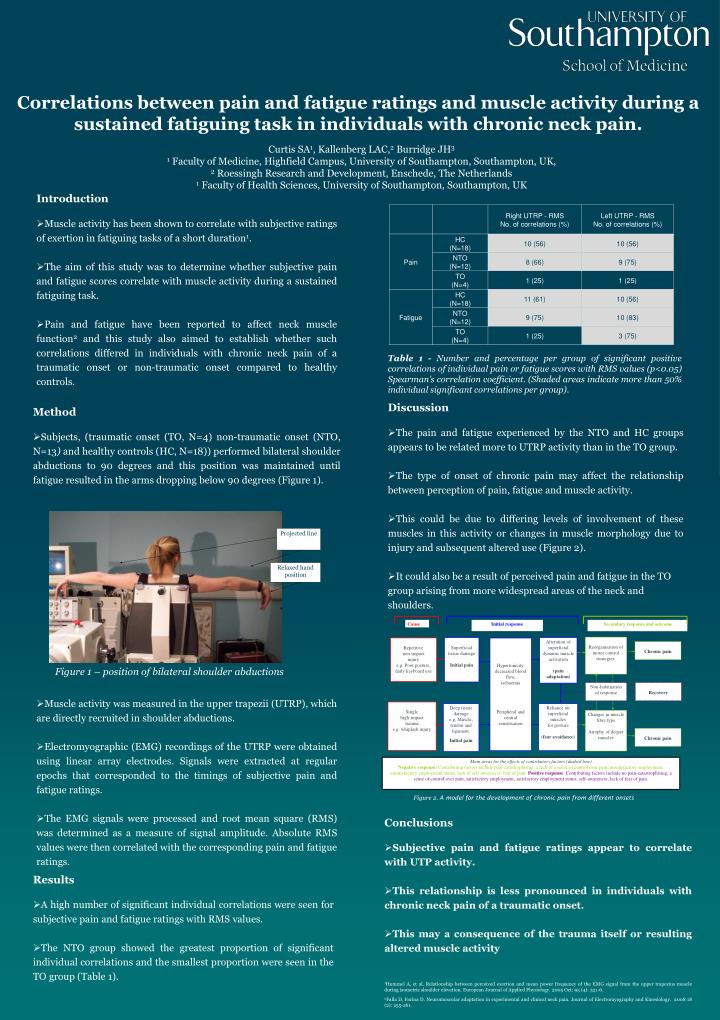
Projected line Relaxed hand position Cause Initial response Secondary response and outcome Reorganisation of motor control strategies. Superficial tissue damage Initial pain Alteration of superficial dynamic muscle activation (pain adaptation) Repetitive non-impact injury e.g. Poor posture, daily keyboard use Hypertonicity, decreased blood flow, ischaemia Peripheral and central sensitisation Chronic pain Recovery Non-habituation of response Single high-impact trauma e.g. whiplash injury Deep tissue damage e.g. Muscle, tendon and ligament. Initial pain Reliance on superficial muscles for posture (fear avoidance) Changes in muscle fibre type Atrophy of deeper muscles Chronic pain Main areas for the effects of contributory factors (dashed line) Negative response: Contributing factors include pain-catastrophising, a lack of a sense of control over pain, unsatisfactory employment, unsatisfactory employment status, lack of self-awareness, fear of pain.Positive response: Contributing factors include no pain-catastrophising, a sense of control over pain, satisfactory employment, satisfactory employment status, self-awareness, lack of fear of pain. Correlations between pain and fatigue ratings and muscle activity during a sustained fatiguing task in individuals with chronic neck pain. Curtis SA1, Kallenberg LAC,2 Burridge JH3 1 Faculty of Medicine, Highfield Campus, University of Southampton, Southampton, UK, 2 Roessingh Research and Development, Enschede, The Netherlands 1 Faculty of Health Sciences, University of Southampton, Southampton, UK • Introduction • Muscle activity has been shown to correlate with subjective ratings of exertion in fatiguing tasks of a short duration1. • The aim of this study was to determine whether subjective pain and fatigue scores correlate with muscle activity during a sustained fatiguing task. • Pain and fatigue have been reported to affect neck muscle function2 and this study also aimed to establish whether such correlations differed in individuals with chronic neck pain of a traumatic onset or non-traumatic onset compared to healthy controls. Table 1 - Number and percentage per group of significant positive correlations of individual pain or fatigue scores with RMS values (p<0.05) Spearman’s correlation coefficient. (Shaded areas indicate more than 50% individual significant correlations per group). • Discussion • The pain and fatigue experienced by the NTO and HC groups appears to be related more to UTRP activity than in the TO group. • The type of onset of chronic pain may affect the relationship between perception of pain, fatigue and muscle activity. • This could be due to differing levels of involvement of these muscles in this activity or changes in muscle morphology due to injury and subsequent altered use (Figure 2). • It could also be a result of perceived pain and fatigue in the TO group arising from more widespread areas of the neck and shoulders. • Method • Subjects, (traumatic onset (TO, N=4) non-traumatic onset (NTO, N=13) and healthy controls (HC, N=18)) performed bilateral shoulder abductions to 90 degrees and this position was maintained until fatigue resulted in the arms dropping below 90 degrees (Figure 1). Figure 1 – position of bilateral shoulder abductions • Muscle activity was measured in the upper trapezii (UTRP), which are directly recruited in shoulder abductions. • Electromyographic (EMG) recordings of the UTRP were obtained using linear array electrodes. Signals were extracted at regular epochs that corresponded to the timings of subjective pain and fatigue ratings. • The EMG signals were processed and root mean square (RMS) was determined as a measure of signal amplitude. Absolute RMS values were then correlated with the corresponding pain and fatigue ratings. Figure 2. A model for the development of chronic pain from different onsets • Conclusions • Subjective pain and fatigue ratings appear to correlate with UTP activity. • This relationship is less pronounced in individuals with chronic neck pain of a traumatic onset. • This may a consequence of the trauma itself or resulting altered muscle activity • Results • A high number of significant individual correlations were seen for subjective pain and fatigue ratings with RMS values. • The NTO group showed the greatest proportion of significant individual correlations and the smallest proportion were seen in the TO group (Table 1). 1Hummel A, et al. Relationship between perceived exertion and mean power frequency of the EMG signal from the upper trapezius muscle during isometric shoulder elevation. European Journal of Applied Physiology. 2005 Oct; 95 (4): 321-6. 2Falla D, Farina D. Neuromuscular adaptation in experimental and clinical neck pain. Journal of Electromyography and Kinesiology. 2008 18 (2): 255-261.