Download
1 / 16
160 likes | 274 Vues
Circle of Care. October 30, 2012. Medicare Payments In 2010. (Percentage) (Dollars in Billions) Inpatient Hospital 39 130 Physician Services 29 96 Outpatient 14 46 Skilled Nursing Facility 8 26

E N D
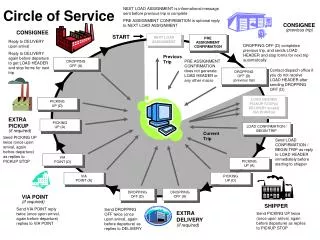
Circle of Care October 30, 2012
Medicare Payments In 2010 (Percentage) (Dollars in Billions) • Inpatient Hospital 39 130 • Physician Services 29 96 • Outpatient 14 46 • Skilled Nursing Facility 8 26 • Home Health Agency 6 20 • Hospice 4 13 • Total 2010 Medicare Expenditures:331 Billion
Program Goals • Reduce preventable hospital readmissions • Safe transition from SNF to home • Provide lower cost, high quality alternative to acute care setting • Provide patient-centered care
SNF Rules Of Participation • Part A (Hospital Insurance) • Qualifying Hospital Stay – Inpatient hospital stay of 3 consecutive midnights • Doctors orders for skilled services • Skilled care required daily • Up to100 day episode of care
Medicare SNF Qualifying 3-Day In-Patient Hospital Stay Required for traditional Medicare Fee For Service under Part A • Exceptions: • Medicare Advantage (Part C) • Tufts, Fallon, Blue Cross Blue Shield, etc. • PACE-Program of All Inclusive Care for the Elderly • SCO (Dual Eligible)-Senior Care Options • MGH Waiver Program
Sensitive Admissions • UTI • Dehydration • Pneumonia • COPD • CHF • Diabetes • Hypertension
Home Health Care Rules Of Participation • Part A (Hospital Insurance) • Services provided under a plan of care established & reviewed regularly by a physician • Require one or more of the following • Skilled nursing care less than 7 days/week • PT, OT or ST • Certified homebound by physician • Up to 60 day episode of care; 30 day window
Home Health Care-Services Not Covered By Medicare • 24 – hour-a-day care at home • Meals delivered to home • Homemaker Services • Personal Care (bathing, dressing and using the bathroom) when this is the only required care
Successful Home Health Care Progams • Communicate with Skilled Nursing Facility and PCP • Provides Consistent Care Givers • Telemedicine – Early symptoms recognition and monitoring
Frequent Causes Of Rehospitalization • Mismanagement of medications • Moderate to severe functional impairment • Inadequate patient/family education • Lack of family safety net • Comorbidities • Patient reluctant to allow care givers in home • Failure to keep follow up appointments • Poor diet, insulin management • Substance abuse
Keys To Safe Transition Home • Discharge planning starts on admit date • Communication with patient, family, PCP and home health agency • Care management meetings with patient, nursing, therapy and case management • Discharge meeting with home health care • Family and Patient education • PCP notification – medication, lab, pending tests and any special needs • Electronic medical records
Life Care Discharge Planning • C.O.A.C. H. • Communicate Expectations • Organize goals • Assign coach • Continued review • Handoff homework
SNF/Home Health Care Agency Coordination Of Care • Home Health Care Agency (HHCA) Case Manager • Reviews patient chart w/SNF Interdisciplinary Team (IDT) • Attends Discharge Planning Meeting at SNF • Coordinates required services (Nursing, Therapy, etc.) with IDT SNF Case Manager • Schedules Home evaluation • Orders DME • Provides education to family care givers
SNF/Home Health Care Agency Coordination of Care • Conducts follow up calls with patient/family (within 48 hours) • Seek feedback-How patient is succeeding at home • Follow up on patient concerns • Provide over the phone education • Assist in providing additional/services if needed • Readmit to facility within 30 days (3 day inpatient hospitalization not required)
Coordinate Circle Of Care Program • Include home health care providers in the discharge process • Educate home health care work force on SNF rules of participation, clinical capabilities, positive patient outcomes • Create an image; the SNF is part of the continuum • Common names; Rehab, Short Stay, Post Acute, Transitional Care • Section 87 State Health Care Reform Law
Coordinate Circle Of Care Program • Coordinate readmission process between home health nurses and SNF • Track & trend outcome data and communicate results with stakeholders • Expand Circle Events to include direct admits from physician offices and emergency rooms when appropriate • Proposed State waiver of qualifying hospital stay