Download
1 / 1
10 likes | 182 Vues
Paraganglioma of T-spine: An Uncommon Cause of Progressive Spinal Cord Compression Monthida Fangtham, MD, Renu Gupta, MD, Nate Ronning, MS, Somnath Ghosh, MD Good Samaritan Hospital of Maryland. Introduction. Hospital Course.

E N D
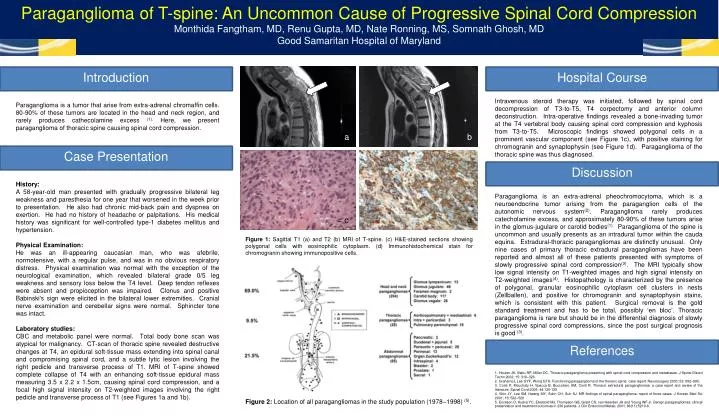
Paraganglioma of T-spine: An Uncommon Cause of Progressive Spinal Cord Compression Monthida Fangtham, MD, Renu Gupta, MD, Nate Ronning, MS, Somnath Ghosh, MD Good Samaritan Hospital of Maryland Introduction Hospital Course Intravenous steroid therapy was initiated, followed by spinal cord decompression of T3-to-T5, T4 corpectomy and anterior column deconstruction. Intra-operative findings revealed a bone-invading tumor at the T4 vertebral body causing spinal cord compression and kyphosis from T3-to-T5. Microscopic findings showed polygonal cells in a prominent vascular component (see Figure 1c), with positive staining for chromogranin and synaptophysin (see Figure 1d). Paraganglioma of the thoracic spine was thus diagnosed. Paraganglioma is a tumor that arise from extra-adrenal chromaffin cells. 80-90% of these tumors are located in the head and neck region, and rarely produces cathecolamine excess (1). Here, we present paraganglioma of thoracic spine causing spinal cord compression. a b Case Presentation Discussion History: A 58-year-old man presented with gradually progressive bilateral leg weakness and paresthesia for one year that worsened in the week prior to presentation. He also had chronic mid-back pain and dyspnea on exertion. He had no history of headache or palpitations. His medical history was significant for well-controlled type-1 diabetes mellitus and hypertension. Physical Examination: He was an ill-appearing caucasian man, who was afebrile, normotensive, with a regular pulse, and was in no obvious respiratory distress. Physical examination was normal with the exception of the neurological examination, which revealed bilateral grade 0/5 leg weakness and sensory loss below the T4 level. Deep tendon reflexes were absent and propioception was impaired. Clonus and positive Babinski's sign were elicited in the bilateral lower extremities. Cranial nerve examination and cerebellar signs were normal. Sphincter tone was intact. Laboratory studies: CBC and metabolic panel were normal. Total body bone scan was atypical for malignancy. CT-scan of thoracic spine revealed destructive changes at T4, an epidural soft-tissue mass extending into spinal canal and compromising spinal cord, and a subtle lytic lesion involving the right pedicle and transverse process of T1. MRI of T-spine showed complete collapse of T4 with an enhancing soft-tissue epidural mass measuring 3.5 x 2.2 x 1.5cm, causing spinal cord compression, and a focal high signal intensity on T2-weighted images involving the right pedicle and transverse process of T1 (see Figures 1a and 1b). Paraganglioma is an extra-adrenal pheochromocytoma, which is a neuroendocrine tumor arising from the paraganglion cells of the autonomic nervous system(2). Paraganglioma rarely produces catecholamine excess, and approximately 80-90% of these tumors arise in the glomus-jugulare or carotid bodies(1). Paraganglioma of the spine is uncommon and usually presents as an intradural tumor within the cauda equina. Extradural-thoracic paragangliomas are distinctly unusual. Only nine cases of primary thoracic extradural paragangliomas have been reported and almost all of these patients presented with symptoms of slowly progressive spinal cord compression(3). The MRI typically show low signal intensity on T1-weighted images and high signal intensity on T2-weighted images(4). Histopathology is characterized by the presence of polygonal, granular eosinophilic cytoplasm cell clusters in nests (Zellballen), and positive for chromogranin and synaptophysin stains, which is consistent with this patient. Surgical removal is the gold standard treatment and has to be total, possibly ‘en bloc’. Thoracic paraganglioma is rare but should be in the differential diagnosis of slowly progressive spinal cord compressions, since the post surgical prognosis is good (3). c d Figure 1: Sagittal T1 (a) and T2 (b) MRI of T-spine. (c) H&E-stained sections showing polygonal cells with eosinophilic cytoplasm. (d) Immunohistochemical stain for chromogranin showing immunopositive cells. References 1. Houten JK, Babu RP, Miller DC. Thoracic paraganglioma presenting with spinal cord compression and metastases. J Spinal Disord Techn 2002; 15: 319–323. 2. GrahamJJ, Lee GYF, Wong GTH. Functioning paraganglioma of the thoracic spine: case report. Neurosurgery 2003; 53: 992–995. 3. Conti P, Mouchaty H, Spacca B, Buccoliero AM, Conti R. Thoracic extradural paragangliomas: a case report and review of the literature. Spinal Cord 2006; 44:120-125 4. Shin JY, Lee SM, Hwang MY, Sohn CH, Suh SJ. MR findings of spinal paraganglioma: report of three cases. J Korean Med Sci 2001; 16: 522–526 5. Erickson D, Kudva YC, Ebersold MJ, Thompson GB, Grant CS, van Heerden JA and Young WF Jr. Benign paragangliomas: clinical presentation and treatment outcomes in 236 patients. J Clin Endocrinol Metab. 2001; 86(11):5210-6. Figure 2: Location of all paragangliomas in the study population (1978–1998) (5).