Download
1 / 148
1.49k likes | 1.75k Vues
Controversies in Melanoma. Prof Ravi Kant , Dr Ajay Yadav, Dr Vivek Gupta, Dr Vishal Gupta, Ms Tanmya Stuti Ravi. Controversies in Melanoma. Biology Detection-Computer, USG, RT-PCR Staging- AJCC 2000 +Prognosis SLN Biopsy + ELND Surgical margins Adjuvant treatment + Vaccines Summary.

E N D
ControversiesinMelanoma Prof Ravi Kant,Dr Ajay Yadav, Dr Vivek Gupta, Dr Vishal Gupta, Ms Tanmya Stuti Ravi
Controversies in Melanoma • Biology • Detection-Computer, USG, RT-PCR • Staging- AJCC 2000 +Prognosis • SLN Biopsy + ELND • Surgical margins • Adjuvant treatment + Vaccines • Summary
Biology of melanoma development and progression
Biology of melanoma • Melanocytes → • Nevus → • Dysplastic nevus → • Radial growth phase → • Vertical growth phase → • Metastases.
Melanoma & Nevi • Class I = Precursor • Class II = Intermediate • Class III = VGP tumorigenic VGP = vertical growth phase
Express adhesions receptors, Integrins, Adherine, and cellular adhesions molecules
melanoma cells express N-adherine instead of E-adherine. • E-adherine allows melanocytes to adhere to keratinocytes, while melanoma cells can not adhere to keratinocytes
Biology- what is new? • PTENpathway = phosphatase and tensin deleted on chromosome 10 → • IGF-1 → Akt / PKB (Oncogene)+PtdIns(3,4)P2→ P13 kinase →growth factor + adhesion receptor (integrin)
Biology – what is new? • Ras pathway→Grb2/Sos →ras →Raf →MEK 1,2 →MAPK 1.2 →TCF/SRF/Elk-1 →Proliferation • As apoptosis is blocked by depriving • Bad & Caspase-9 from p13 kinase • Apoptosis turned into growth
Nevus • Proliferative lesion of melanocytes • Scattered along basal layer • Acquired - mostly • congenital
Naevi : types • Lentigo Flat • Junctional • Compound – slightly elevated • Intradermal – papillomatous
Naevi: Lentigo simplex-1 • Pigmented macule, <5mm, jet black color • In infants & children • Melanocytic proliferation along basal layer
Naevi: Lentigo simplex-2 • Abundant melanocytes along basal layer • Associated with Peutz-Jegher syndrome • P-J syndrome = hamartomatous polypes in GIT +naevi in oral & buccal mucosa
Naevi: Junctional • Next stage after lentigo • Macular lesions, < 7mm • Less deeply pigmented than lentigo • Homogenous brown black areas • Melanocytic proliferation along basal layer • Highest malignant potential
Naevi: Compound • Next stage of maturation of junctional naevi • In children & adolescent • Pale brown & papular • Junctional + dermal component
Naevi: Intradermal • Last stage in maturation • Mostly after 30 years of age • Flesh colored papule with little pigment • Melanocytes confined to dermis only
Blue naevi • Benign melanocytic naevi • Slate blue color • Two types : common & cellular
Common Blue naevi Mostly in scalp & dorsum of hand, feet • Dermal collection of spindle melanocytes • F > M , max. in 4th decade
Blue naevi: Cellular type • Uncommon • F > M • > 50% in sacrococcygeal area& buttock • < 1% under go malignancy • Rx : simple excision
Nevus • Common • Atypical • Congenital • Spitz • Familial
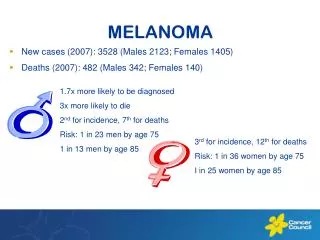
Malignant Melanoma • Arises from transformed melanocytes of epidermis • Accounts for almost all deaths from skin cancer • 4 fold increase in incidence in Australia
Melanoma : Risk Factors-1 • Congenital naevi >5% BSA, 1000X • Previous melanoma • Family history • 5 naevi > 5mm (Common nevi) • 50 naevi > 2mm (Common nevi)
Melanoma : Risk Factors-2 • Dysplastic nevi, Atypical= 2X for single; 12X for >10 • Family history Atypical =37-148X • Dysplatic naevi syndrome
Melanoma : Risk factors-3 • White race, • Red hair, • Blond hair, • Blue eyes • Poor tanning ability, • Sunburns during childhood • Albinism
Melanoma : Risk factors-4 • Freckles • Equatorial latitude • Xeroderma pigmentosa • Psoralen sunscreen • Tanning salons • Junctional naevi
Melanoma : Risk factors-5 • Spitz Nevi= benign except when • >10 y age • +ulceration • >1cm • Involve subcut fat • Mitotic activity >6/mm2
Melanoma : Risk factors-6 • Familial syndromes • B-K nevus syndromes • Atypical nevus • CDKN2A mutation • CDK4 mutation
DD • Pigmented Basal cell CA • Seborrheic keratitis • Solar lentigines • Atypical nevi
MM: Clinical features • Lentigo maligna : Hutchinson's freckle (7-15%) • Superficial spreading : most common (60-70%) • Nodular : 12-25% • Acral lentiginous • Amelanotic
1. Superficial spreading Melanoma • Most common type 70% • Occur any where on skin except hands & feet • Usually > 5 mm , flat • Variegated color pattern • Irregular edge with areas of regression • Long radial growth phase
2. Nodular Melanoma • Most malignant • Younger age group • Any part of the body • raised and always palpable with sharp irregular border • Blue, black or gray color • Lack of radial growth phase
2. Nodular Melanoma • Second most common 15-30 % • Rapid onset • ♂>♀
3. Lentigo maligna Melanoma • Hutchinsons melanotic freckle • Least common type 5% • Most commonly on face of elderly • Begins as irregularly pigmented ,flat, brown macule • quite large at the time of diagnosis late invasive growth phase • Good prognosis
4. Acral lentiginous • Uncommon 1-3% • Palm, sole, heel & subungual • More common in dark skin persons • Subungual –common in big toe or thumb • Poor prognosis , 29%@20Y • 70% ulcerate, 74% >1.5 mm
4. Acral lentiginous-risk factor • >50 y age • >3mm width, variegated border • Extension of pigment in to nail bed/ nail fold • Dark complexioned patient
5. Amelanotic Melanoma • Desmoplastic, 1.7% • H&N • Pink, reveal some pigment on close inspection; Stain+ with S-100 • Worse prognosis • Often present with regional lymph nodes metastases
5. Amelanotic Melanoma • Locally aggressive • Known for local recurrences • Stain ► S-100
MM : spread • Local extension • Blood stream : lung, liver, brain, skin • Lymphatic : • embolisation, permeation • satellite nodule • in-transit nodule
Controversies in Melanoma • Biology • Detection-Computer, USG, RT-PCR • Staging- AJCC 2000 +Prognosis • SLN Biopsy + ELND • Surgical margins • Adjuvant treatment + Vaccines • Summary
MM : Diagnosis • Signs of transformation of mole in to MM • Major • Change in size, shape, color • Minor • Inflammation, itching • Crusting or bleeding • > 5mm diameter
MM: Diagnosis • A : Asymmetry • B : irregular border • C : color variegation • D : diameter > 5 mm • E : enlargement or evolution
Detection- Vision • A = asymmetry • B = border irregularity • C = color variegation • D =diameter > 6mm • E = elevation, enlargement, evolutionary changes • F= any funny change
Detection- Vision • Change in size • Change in shape • Change in Color • Inflammation • Crusting / bleeding • Sensory change • > 7mm in size enlargement
Detection- Digital Vision • Epiluminescence microscopy • Dermatoscopy • Surface microscopy • Incident light microscopy • Can see the dermis, epidermo-dermal junction
Melanin pigment network Black dots Globules Streaks Radial streaming Blue-white milky veils Pseudopods Pseudo network Structure less area Melanin reticulum Epidermo-dermal junction Multiple brown dots Epiluminescence microscopy-ominous signs