Download
1 / 57
650 likes | 1.38k Vues
Urine Appreciation 101. Jason M. Eberhardt, DVM, MS, DACVIM. Why Urine?. “Urine…the wine of the body” Dr. Wilke “God made urine gold for a reason” Dr. Barges “Don’t ever give me another set of blood work without a urinalysis” Dr. DeClue to an intern. The Routine Urinalysis.

E N D
Urine Appreciation 101 Jason M. Eberhardt, DVM, MS, DACVIM
Why Urine? • “Urine…the wine of the body” • Dr. Wilke • “God made urine gold for a reason” • Dr. Barges • “Don’t ever give me another set of blood work without a urinalysis” • Dr. DeClue to an intern
The Routine Urinalysis • Should be performed…“routinely” • It’s part of a sentence • CBC, Chemistry, UA. • Provides invaluable data of overall health • Regardless of clinical status of patient
Sample Collection • Sample Method Matters • Cystocentesis is typically preferable • Hematuria? • Try to evaluate fresh samples • Can affect interpretation • Warm refrigerated samples prior to evaluation
Aspects of a UA • Physical Properties • Appearance • Specific gravity • Chemical Properties • pH, Protein, Glucose, Ketones, Blood, Bilirubin, Leukocyte Esterase Rxn • Urine Sediment Examination • Specific tests
Appearance • Why is urine yellow? • Depth of color is RELATED to volume and concentration • YELLOW URINE DOES NOT MEAN CONCENTRATED URINE! • What about abnormal pigmenturia???
Red to reddish-brown • RBC’s • Hemoglobin • Myoglobin • To distinguish – centrifugation • Hematuria will clear • Hemoglobinuria/myoglobinuria will not • Key in determining further diagnostic plan
Causes of hematuria • Trauma • Traumatic collection -Iatrogenic increase without gross change is common, Renal Bx, Blunt trauma • Urolithiasis • Neoplasia • Inflammatory Dz • UTI, FLUTD/FUS, Drug induced (ie cyclophosphamide induced cystitis) • Parasites (Dioctophyma renal, Capillaria plica) • Coagulopathy - Warfarin toxicity, DIC, Thrombocytopenia • Renal infarction • Renal pelvic hematoma • Vascular malformation – • Renal telangiectasia (Welsh Corgi’s), Idiopathic renal hematuria • Estrus • Inflammation, neoplasia, trauma to genital tract
Site of origin… • Urinary tract origin • Kidneys, ureters, bladder, urethra • Genital tract contamination • Prostate, prepuce, vagina
It’s not blood… • Hemoglobinuria • Common Abnormal pigment • Serum is typically pink • Usually indicates hemolysis • Myoglobinuria • Serum is typically Clear • Usually indicates severe rhadomyolysis
Other changes • Yellow brown/green • Bilirubin – Pre-hepatic, Hepatic, Post-hepatic • Cloudy-white • Increased cellular elements, crystals, mucus • Brown-black • Post Oxyglobin administration • Smell… • Ammonia produced by urease-producing bacteria
Specific Gravity • Remember dipsticks are unreliable • Accurate readings between 60-100° • “Normal” USG • No such thing… • Dehydration • Dog >1.030 • Feline >1.035
Isothenuria • 1.008-1.012 • Neither concentrated nor diluted • Owner may or may not report PU/PD • Recheck morning sample if no clinical signs • Accurate history!
Hypothenuria • <1.007 • Indicates renal ability to dilute glomerular filtrate (renal failure is not present?) • Persistent hypotheuria • Atypical/early renal failure (typically 1.006-1.007) • Cushing’s dz* • DI • Psychogenic
PU/PD • Go back to basics • History, History, History • Is the patient drinking too much causing them to urinate more or… • Is the patient urinating more so they have to drink more…
PU/PD • Primary polydipsia • Diabetes insipidus • Resistance to ADH • Osmotic diuresis • Medullary washout • Misc.
Approaching PU/PD • Common things are common… • Dogs: CKD, DM, Cushing’s • Cats: CKD, DM, Hyperthyroidism • CDI, Primary NDI, Psychogenic are rare! • Initial plans should be simple and safe • Water deprivation does not meet this criteria • Use specific test results to r/o specific dz • Urine culture for pyelonephritis • Look it up and mark them off!
Urine pH • Normal is between 5.0-7.5 • Some resources list up to 8.5 • Varies with diet and acid-base balance • Dipsticks have moderate to poor correlation with pH meters
pH Continued • Refrigeration for up to 24 hours does not clinically impact pH • However, leaving at room temperature leads to CO2 contamination • IS NOT RELIABLE INDEX OF BLOOD pH • Hypochloremic metabolic alkalosis can have aciduria
Causes of urine pH alterations • Low pH • Meat ingestion, acidosis, hypochloremic metabolic alkalosis, diarrhea, starvation, pyrexia, urine acidifiers, proximal renal tubular acidosis • High pH • Postprandial alkaline tide, ingestion of alkali (bicarb or citrate), alkalosis, UTI w/urease-producing bacteria (usually Staph or Proteus spp.), high vegetable/cereal diets, distal renal tubular acidosis
So… • It can be a challenge to determine the exact significance of urine pH (especially in a single sample and/or not comparing to blood pH) • Persistent alkalosis could prompt further diagnostics (ie urine culture) • pH can affect other urinalysis findings • Glucose (Low pH) • Protein (high pH) • Crystal formation
Proteinuria • Diagnostic marker • CKD • Systemic disease • Potential for progression • Semi-quantitative screening methods • Dipstick • Sulfosalicylic acid turbidimetric test (SSA)
Dipsticks and Proteinuria • Primarily measures albumin • False positives • Alkaline urine • Active sediment (“Post-renal”) • Left in contact with stick too long • False negatives • Bence-Jones proteins, low specific gravity, proteinuria <30 mg/dl
SSA Test • Urine + 5% SSA • Grade turbidity on scale 0-4 • SUBJECTIVE • Detects albumin, Bence-Jones, globulins • FP: Drugs (including Penicillins and Cephalosporins) • Can detect >5 mg/dl
Microalbuminuria test • Detects >1 mg/ml • If dipstick and SSA are positive • What’s the point??? 1) Equivocal/conflicting results? 2) More sensitive test is desired? 3) Familial risk
USG and Proteinuria • Most resources cite that if USG >1.035 then 1+ protein is “normal” • At what USG is trace to 1+ protein NOT normal • ???
Urine protein:creatinine ratio • What is normal??? • <0.5 Dogs; <0.3 Cats • 0.5-1.0 Mild • >1.0 – 2.0 Moderate • >2.0 Severe (typically glomerular dz)
Localization • Physiologic/Functional • Technically a “renal” cause of proteinuria • Strenuous exercise, seizures, fever, extreme environmental exposures • Transient, low grade & does not require specific tx • Pathological • Extra Urinary • Pre-renal vs. Genital system • Urinary • Renal vs. Post-renal
Extra Urinary Causes • Genital tract inflammation • Comparison of cysto. vs. free-catch samples • Dysproteinemias • Bence-Jones proteins • Dipstick negative, positive SSA • Hemoglobin/myoglobin
Urinary Causes • Rule out “post” renal causes first • Infection, neoplasia, urolithiasis • Primary Renal • Glomerular • Most common cause of persistent, high-magnitude • Tubular-interstitial • May also have other findings of tubular disorder
Practical evaluation • Evaluate History and PE findings • Go back and look at blood work • Proteins, renal values, cholesterol, electrolytes • Evaluate other UA findings • Further diagnostics • Urine culture • Infectious dz testing as appropriate • Blood pressure • Abdominal imaging • Endocrine testing as appropriate • Chest radiographs
Concurrent disease • Common to find concurrent medical conditions • Neoplasia • Infection (dental dz, heartworm, etc.) • Immune mediated dz • Systemic hypertension • Viral (cats) • 43% of patients with severe proteinuria do not have an identifiable concurrent disease (Cook and Cowgill, 1996).
When to treat? • Recommendations continue to change… • Depends on concurrent disease(s) • Azotemia vs. Non-azotemic patients • Azotemia: Consider even if mild? • ACVIM Consensus • >0.5 dogs; >0.3 Cats • Non-azotemic: If persistently moderate-severe
Therapy Considerations • Discontinue renal toxic medications • Tx underlying conditions • Reduced (not necessarily low) protein diet • ACE inhibitors • Low dose aspirin supplementation • Only if hypoalbuminemic? • Fatty acid supplementation • Always investigate/address hypertension • Immunosuppression???????
ACE Inhibitors • It is important to start low and gradually increase with monitoring • Blood pressure • Renal Values • Electrolytes • Degree of proteinuria
Glucosuria • Glucose reabsorption occurs in the proximal tubule • Typically occurs when renal threshold is exceeded • >180 mg/dl Dogs • >300 mg/dl Cats
They’re not diabetic… • Recheck dipstick 1st • Abnormal proximal tubular function • Simple vs. Complex • Toxin • Aminoglycoside toxicity • Fanconi’s disease • Primary renal glucosuria
If repeatable… • Presumptive proximal tubular dysfunction • Further evaluation • Repeat hx • Evaluate renal function • Urine culture • Abdominal ultrasound • Investigate for complex renal disorders
Ketonuria • Ketones produced by lipolysis • Occurs earlier in young animals • Dipsticks react to acetoacetate and acetone • Positive • DM, Drugs, prolonged starvation, low carb diets (Atkin’s diet), persistent fever, persistent hypoglycemia, glycogen storage dz
Bilirubin • Dogs have lower renal threshold • Male dogs can have 1+ in concentrated urine • Positive is nearly always important in cats • All the same causes as hyperbilirubinemia • Will see prior to serum increases • Can help differentiate lab error on chemistry
Misc. dipstick results • Leukocyte esterase reaction • Low sensitivity in dogs • High number of false negatives • Low specificity in cats • High number of false positives • Rely on high quality urine sediment exam • Urobilingen and Nitrites – WWHD???
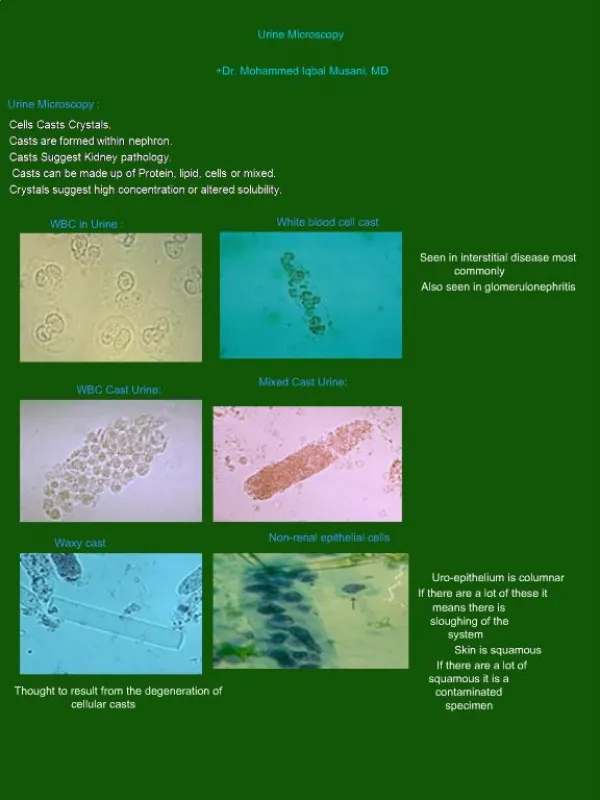
Sediment - Cells • RBCs, WBCs, Bacteria • Epithelial Cells • Both squamous and transitional cells can be found in sediment • Typically of little diagnostic significance • Neoplastic cells • Fresh samples • New methylene blue or Wright’s-Giemsa stains • Difficult to differentiate from “reactive” changes
Bladder Tumor Antigen Test • Detects a glycoprotein antigen complex associated with bladder cancer (humans) • Sensitivity 90%; Specificity 78% • False positives • Proteinuria, glucosuria, pyuria, hematuria • Specificity only 41% in urinary tract dz other then TCC • PPV 3% (NPV 100%)
Cylindruria • Supports presence of renal disease • Type can give indication to disease process • Composed of aggregated proteins or cells • Form in ascending limb of Henle and distal tubules • Best evaluated on fresh samples
Hyaline Casts • Pure protein precipitates • Mucoprotein + albumin • Actually dissolve rapidly in dilute or alkaline urine • Typically seen in diseases that cause proteinuria • Can also be seen with diuresis, correcting dehydration • Consider further evaluation for proteinuria???
Other “casts” of characters • Granular • Degenerating cells, proteins and other “stuff” • Supportive of acute tubular injury • Toxic, Ischemic • Cellular • WBCs, Epithelial, RBCs • Pyelonephritis, acute tubular injury • Waxy casts • “Old” granular casts
“Casting your lot” • Presence of casts are often the first sign of tubular injury • EVALUATE FRESH SAMPLES • Useful in monitoring for toxicity • Aminoglycosides • Amphotericin • Ingestions
Crystalluria • Formation dependant on pH, temp. & USG • Commonly present, seldom significant • Crystalluria does NOT correlate well with urolithiasis**