Download
1 / 43
430 likes | 566 Vues
Common Practice, Fatal outcome. Dr MC Luk Dr KB Tai 20/1/2009. Mr YP Man M/54, chronic smoker PHx: ? Thyrotoxicosis > 10yrs, on over-the-counter medications, no regular fu/Tx HPI: c/o palpitation, SOB and orthopnoea for few months decreased exercise tolerance .

E N D
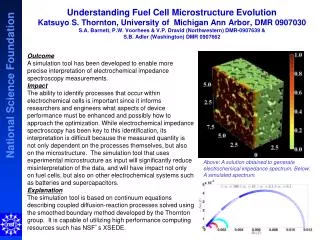
Common Practice, Fatal outcome Dr MC Luk Dr KB Tai 20/1/2009
Mr YP Man • M/54, chronic smoker • PHx: • ? Thyrotoxicosis > 10yrs, on over-the-counter medications, no regular fu/Tx • HPI: • c/o palpitation, SOB and orthopnoea for few months • decreased exercise tolerance
P/E on A&E admission • Temp 36.7, Bp 121/89, • p164/min, • SpO2 96% RA , • Thin, • Goitre + • Tremor +
Ix: • ECG :Fast AF, no ischemic change • CBP: WBC 8, Hb 14, Plt 236 • RFT 138/4.3/9/84 • CXR
Tx in A&E at 12:40 • Inderal 10mg stat po • NS 500ml Q8hr IV • Admitted Med
Palpitation, SOB, orthopnoea 2-3/12 • Hot intolerance • Not on any medications for mths • No fever • No past hx of heart dz • P/E on ward admission at 15:00 • Fully conscious • Bp 115/89, p 147/min, SpO2 96% 2L O2 • Temp 37.4, • no Ankle edema, • CVS: PSM apex radiate to axilla • Chest :clear
Provisional dx • Fast AF • ?Thyrotoxicosis • ?CHF ppt by fast AF, cardiomegaly and bil. pleural effusion • Ix: • TSH • Echo • Tx given: • Digoxin 0.25mg po q8hr x3 • Carbimazole 10mg daily
Progress: • at 21:00 • Bp 132/95, P 132, SpO2 96% on 2L NC • ↑ Carbimazole 10mg tds • + Inderal 10mg tds • at 02:10 • Bp 153/115, p 122/min, SpO2 88% 2L • Resp distress • Rechecked SpO2 86% 10L NRM • Transferred to CCMU
at 02:44, CCMU • Bp 150/80 • P 156/min • RR 46/min, • Chest: Bil. LL crep. • I stat: type I resp failure, SaO2 87% on 10L NRM • Failed CPAP and intubated for MV • CXR
at 04:00 • Bp 100/55, p 160/min, • U/O: 5ml/hr • Echo: global hypokinesia, impaired LVEF 30%, mod-severe MR/TR, dilated RA/RV, PASP 39mmHg • started on Amiodarone infusion + IV Hydrocortisone 100mg q8hr
Started noradrenaline then adrenaline infusion for hypotension • PEA at 7am • Not responded to CPR • Certified death • Refer coroner
Ix result : • TSH < 0.02 • FT4 >100 • Waived • Cause of death : • 1)Thyrotoxicosis, 2)CHF
Effects of thyroid hormone on cardiovascular hemodynamics • Thyroid hormone (T4/T3) • ↑ myocardial contractility • Change in the synthesis of myosin heavy chain protein from the β to the α form • ↑ transcription of the Ca ATPase gene, • enhanced Ca and glu uptake • ↓ afterload • Direct effect on vascular smooth muscle • ↑ preload as blood volume is expanded • ↑ angiotensin converting enzyme • ↑ erythropoietin • ↑ resting heart rate • More rapid diastolic depolarisation and shortening of the action potential of sinoatrial cells • Enhance sensitivity to catecholamines • ↑ cardiac output
Changes in Cardiovascular Function Associated with Thyroid Disease Klein I and Ojamaa K. N Engl J Med 2001;344:501-509
Thyrotoxicosis and its cardiovascular complications • Atrial fibrillation (AF) • the most well-known cardiovascular complication in thyrotoxic patients • occurs in 5 to 20 % of patients with thyrotoxicosis • 13 % of patients with unexplained AF have biochemical evidence of thyrotoxicosis • The prevalence of AF increased with age in thyrotoxic population as in general population. • The prevalence of AF was higher among thyrotoxic men than women
62% thyrotoxic patients with AF had spontaneous sinus conversion within the first 3 to 4 months after euthyroidism, even without anti-arrhythmic agents. • For those thyrotoxic patients with persistent AF after euthyroidism achieved, DC cardioversion is highly effective for sinus conversion (~90%) and sinus rhythm maintenance rates were exceedingly high (56% at tenth year) compared to nonthyrotoxic AF population whom underwent cardioversion
Congestive Cardiac Failure • May be contributed by • Fast AF • Diastolic dysfunction • Pre-existing heart dz • Poor cardiac reserve • thyrotoxic patients exhibited a high LV ejection fraction at rest but paradoxically the EF fell significant during exercise. • “tachycardia induced cardiomyopathy”
Siu and colleagues studied 591 consecutive patients with primary hyperthyroidism. • CHF was the presenting condition in 34 patients (5.8%) with hyperthyroidism. • The presence of atrial fibrillation at presentation (OR 37.4, 95% CI 9.72 to 144.0, p<0.001) was an independent predictor for the occurrence of CHF. • Of the 34 patients with CHF, 16 (47%) had systolic left ventricular dysfunction with left ventricular ejection fraction (LVEF)<50%. • predominantly male. • had a lower serum thyroxine level than patients with preserved left ventricular systolic function. • In these patients, LVEF and NYHA functional class improved significantly 3 months after achieving euthyroid status. • Systolic left ventricular dysfunction (mean (SD) LVEF 38 (4)%) persisted on long-term follow-up in five patients: no clinical parameter could be identified to predict the occurrence of this persistent cardiomyopathy (p>0.05). Siu CW, Yeung CY, Lau CP et al.Heart 2007;93:483
Pulmonary Hypertension • Increasingly recognized as a rare cause of pulmonary hypertension • Possible mechanism have been put forwards to explain this association: • 1) high cardiac output in thyrotoxic state, • 2) elevation of pulmonary vascular resistance. • ?reversible • the pulmonary pressure fell back to normal after euthyroidism achieved.
Siu and colleagues performed serial echo. exam. in 75 consecutive patients with hyperthyroidism at baseline and 6mths after initiation of antithyroid tx. to estimate PASP, CO, total vascular resistance and LV filing pressure. • Results were compared with 35 age- and sex-matched healthy controls. • All patients had normal LV systolic function. • 35 (47%) had PHT with PASP ≥ 35mmHg. • No sig. differences in the clinical characteristics. • Asymptomatic • Follow-up echo was performed in 27/35 who had achieved a clincially and biochemically euthyroid state at 6mth • The mean PASP decresed from 47±2 to 34 ±2 mmHg (P<0.01) Siu CW, Zhang HX, Yung C et al. JClin Endo Meta 92:1736-1742,2007
Medical treatment • Therapy to control the thyroid • Thionamides (PTU, Carbimazole) • Iodinated medications (Iopanoic acid, Lugol’s solution) • Lithium carbonate • Therapy to block conversion of T4 to T3 • PTU • Iopanoic acid • Propanolol • Corticosteriods • Therapy to enhance clearance of thyroid hormones • Gastrointestinal clearance • Cholestyramine • Blood clearance • Plasmaphresis/hemodialysis/hemoperfusion • Therapy to block the effects of thyroid hormones • Beta blockers • Corticosteriods • Supportive measures • Tx of CHF • Antipyretics • Correction of dehydration • Antibiotic for precipitating infection
Thionamides: Propylthiouracil (PTU) and carbimazole • Both are effective and can act rapidly to block iodide organification and formation of thyroid hormone • PTU may have the added benefit of inhibiting T4 to T3 conversion at high dose (e.g. 200mg q4hr) • No parenteral formulation is available but both can be given as rectal suppositories • Both cannot block release of the preformed thyroid hormone stores in the colloid space.
Iodines and Lithium carbonate inhibits the release of preformed thyoid hormone stores in the colloid space • Usual dosage: • Iopanoic acid 1gm q8hr for 1st day then 500mg bd po • Lugol’s solution 4-8 drops q6-8hrs po • Lithium carbonate 300mg q6hr po ,dose adjusted to maintained serum levels ~1mEq/L
Cautions: • Thionamides must be given before iodines as monotherapy with iodides results in the initial formation and release of new thyroid hormone and can thereby worsen the thyrotoxicosis • Therapy with iodides may prevent future therapy with radioiodine for several mths
Cholestyramine • Thyroid hormone undergoes resorption in the distal small bowel through the enterohepatic circulation. • Cholestyramine will bind thyroid hormones in the GIT ,resulting in a modest reduction of circulating thyroid hormone level • Dose : 4gm tds po
Corticosteroids: • Reduce conversion of T4 to T3 , block effects thyroid hormone in the target tissues. • Higher incidence of concomitant adrenal insufficiency in patients with Graves’ dz (so please also check spot cortisol before initiation of therapy) • Hydrocortisone 100mg q8hr iv
Digoxin • Higher dose is required for thyrotoxic AF • ↑ renal clearance • ↓ sensitivity of the hyperthyroid heart
Amiodarone • an iodine-rich benzofuran. • It is a safe and effective agent for chemical cardioversion of atrial fibrillation, even when the dysrhythmia is refractory to other drugs.
2nd line treatment • amiodarone-induced hyperthyroidism (AIT) range from 2% to 10% and vary directly with duration of treatment.
Beta blockers • All beta blockers effectively ameliorate s/s of thyrotoxicosis and control heart rate. • Propanolol (Inderal) has been used most frequently because of its effects on peripheral conversion of T4 to T3 • Esmolol IV infusion 0.05-0.1 mg/kg/min • ultra-short acting (half-life of 9 min) facilitates rapid titration of β-adrenoceptor blockade
“Initial treatment of patients with the entire spectrum of cardiac-related symptoms and signs of hyperthyroidism, from sinus tachycardia and exertional dyspnea to heart failure, should include a Beta-adrenergic- receptor antagonist and the goal of therapy is to lower the heart rate to nearly normal” Klein I and Ojamaa K. N Engl J Med 2001;344:501-509
“Double-edged Sword” • Invasive monitoring in hyperthyroid patients with cardiac failure has demonstrated depressed myocardial function in response to β-adrenoceptor blockade, as evidenced by decreased stroke volume and increased pulmonary artery diastolic pressure.
Use or Not use Beta blocker • Rate reduction in diastolic dysfunction • Close monitoring • Ultra short acting
Thyrotoxic Heart disease Ngo AS, Lung T, Resuscitation 2006; 70(2): 287-290 • Fatal thyrotoxic cardiomyopathy in a young manM. C. Soh ,M. Croxson, BMJ, 2008; 337(nov28_1): a531 - a531. • Cardiovascular Collapse Associated with Beta Blockade in Thyroid StormR. Dalan, M. Leow , Exp Clin Endocrinol Diabetes 2007; 115: 392-396
Summary • Cardiovascular complications of thyrotoxicosis • Atrial fibrillation • CHF • Pul. HT • ? Reversible • Medical Treatment • PTU Vs Carbimazole • Adjunct treatment for severe thyrotoxicosis • Iodides, lithium, cholestyramine, hydrocortisone • Beta Blocker = “double-edged sword”