Download
1 / 57
570 likes | 971 Vues
Title V - Maternal and Child Health Block Grant to States and Territories. Nan Streeter MCH Director Utah Department of Health February 2005. Origin of Title V.

E N D
Title V - Maternal and Child Health Block Grant to States and Territories Nan Streeter MCH Director Utah Department of Health February 2005
Origin of Title V Title V of the Social Security Act has provided a foundation and structure for ensuring the health of mothers and children in this country for more than 65 years.
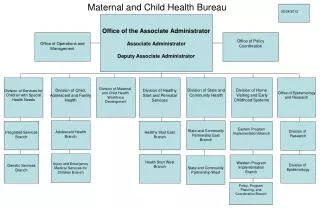
Title V Today Today Title V is administered by the Maternal and Child Health Bureau (MCHB) in the Health Resources and Services Administration (HRSA)
State MCH Block Grant In most states, the Title V Block Grant funding is awarded to the State Department of Health • Some states are organized differently, such as Department of Health and Human Services, or Department of Social Services
State MCH Block Grant Some states are organized such that the “MCH” part and the “CYSHCN” part are in two different state agencies In this case, the Title V funding is usually split between two agencies
State and Territorial Agencies • Often state agencies are responsible for oversight of Title V, as well as other programs that address needs of mothers and children, such as • WIC • Immunizations • Part C • Etc
Providers of Public Health Services for Mothers and Children • State agencies • Managed care organizations • Local health departments • Community health centers • Private providers
Block Grant Requirements • Submission of annual plan and report that details how Title V agency will address the National and State Performance Measures
National Performance Measures • Pregnant women receiving early prenatal care • Very low birth weight births (babies weighing less than 3 lbs.) • Very low birth weight infants delivered at high-risk facilities • Breastfeeding at hospital discharge
National Performance Measures • Newborns screened for hearing before hospital discharge • Newborn blood screening • Age-appropriate immunizations • Protective sealants on children’s molars
National Performance Measures • Children without health insurance • Medicaid eligible children receiving service paid by Medicaid • Teen births (15 to 17) • Deaths to children caused by motor vehicle crashes • Suicide deaths among youths 15-19
National Performance Measures • Family involvement in decision making for children with special health care needs • Coordinated, ongoing, comprehensive care within a medical home for children with special needs • Adequate private and/or public insurance for CSHCN
National Performance Measures • Community-based service system for CSHCN is organized so it can be use easily • Youth with special health care needs who receive services necessary to make transitions to adult life
Smoking - pregnancy, youth Oral health Mental health Unintended pregnancy Well child care Family violence Asthma Birth defects Quality child care Cause-specific mortality Alcohol and drug use Nutrition Blood lead Obesity Breastfeeding State Performance Measure Examples
National Outcome Measures • Infant mortality • Infant death rate disparity • black versus white • Child mortality
Federal Funding Requirements • States and territories are required to allocate federal funding by the 30-30-10 distribution • States are also required to provide non-federal match funding to maximize federal dollars serving mothers and children
Allocation of Funding for Title V Agencies Title agency funding varies from Palau Guam $162,320 $901,847 Alaska California $1.2 million $48+ million
Sources of Other Funding for Title V Programs • Other federal funds – grants • State funds • Private funding • Local MCH funds – city/county • Program income funds – clinic services
Federal Funding Requirements • States have encountered challenges in meeting the non-federal matching requirement due to significant state budget cuts with the economic downturn after 9-11
Federal Funding Requirements • States and territories are required to allocate federal funding by the 30-30-10 distribution, but • How do we ensure that we have healthy mothers?
Federal Funding Requirements • Some restrictions on Title V funding • No building improvement, purchase of land, etc. • Limited inpatient services • No cash payments to recipients of services
Allocation of Funds by States • States and territories are given broad flexibility in how the federal funds are used • Title V does not cover all programs and services to mothers and children that a state provides, but Title V serves as the structure for states to be able to provide them
Allocation of Funds by States • States allocate the funding in very different and innovative ways • Many states have shifted their resources from providing health care directly, such as provision of prenatal care or well child checkups
Allocation of Funds by States • States may shift funding to local health agencies, such as local public health departments or community health centers so that they can provide the health care services to mothers and children in their communities • State agencies contract with local public health departments and community health centers to expand their ability to serve women and children in need
Title V in States • Title V funds may not go directly to finance specific services or programs, but may provide resources to make these happen
Allocation of Funds by States • States may choose to allocate the funding to support the “population” rather than smaller number of individuals thus impacting more mothers, children and children with special health care needs • Example of state services • State Maternal and Infant Programs that provided prenatal and postpartum care to high risk women and pediatric care to their children
Allocation of Funds by States • Shift to population-based services - services that address the entire population of mothers and children • Educational programs - 13 / 13 “Danger signs of pregnancy” • Hotlines – information on where and how to get services
Allocation of Funds by States • Newborn screening – hearing and blood spot testing • Immunizations • Programs that promote the importance of good oral health, good nutrition and physical activity
Allocation of Funds by States • Investigation into issues that lead to poor health for mothers and children • Late or no prenatal care – associated with higher prematurity and infant death rates (13 / 13 campaign) • Mortality review – helps identify “systems” issues, such as hospitals keeping very high-risk pregnant women rather than transferring them to a perinatal center
Allocation of Funds by States • Establishing policy and standards • Hospital rules that require hospitals to meet certain requirements for high risk perinatal care • Death reviews that reveal issues in systems of care, such as physicians not consulting with specialists when faced with high risk pregnancy, or child who was treated inappropriately for infection
Allocation of Funds by States • Services that “enable” mothers and children to get services, such as • Transportation to medical appointments • Respite care for parents of children and youth with special needs
Allocation of Funds by States • Support services • Child care services so parent can get to medical appointments • Health care coverage
Why States Allocate Funds the Way They Do • Title V funds state work that builds the “infrastructure” in the state for addressing the health needs of mothers and children • If states used all of the funding for services for those in need, there would never be enough funding and factors related to poor health outcomes would not be addressed
Why States Allocate Funds the Way They Do • Infrastructure = the foundation on which the rest of the health care relies • Think of infrastructure as a house that should be efficient • You pay for the house, but discover that it has some problems that impact your monthly bills • Leaky faucet – increases your water bill = money lost • Drafts in the house – increases your electric and gas bills = money lost
Why States Allocate Funds the Way They Do • You can continue to pay out the extra income every month for the increased water use and increased energy use, or you can invest money to try to fix the problems • Hire a plumber to fix the leak – may mean you have to put out more money at first to fix the leak, such as buying a new faucet • Hire someone to better insulate your house – this may mean that you need new windows that don’t leak
Why States Allocate Funds the Way They Do • Identifying needs, such as late entry into prenatal care and developing strategies to address • Information systems – CHARM, IBIS • Quality Assurance – UPIQ (Vermont and North Carolina)
Example of State Allocation of Funds • In Utah we closed our M&I Program in 1995 because the services provided were no longer unique, we were serving small numbers of families per year at great cost
Example of State Allocation of Funds • When we closed the Maternal and Infant Program • We were only serving 200+ families each year • Funding for this program amounted to approximately $500,000 per year
Example of State Allocation of Funds • We reallocated the funding to three initiatives: • Increased Medicaid reimbursement rates for prenatal enhanced services, such as care coordination • Contract with local health department and community health center to provide prenatal care • State PRAMS Program which then evolved into a CDC funded program
Impact of Reallocation of Funds • Increased Medicaid reimbursement for enhanced prenatal services – aim was to increase access to these services by bringing reimbursement rates to a more reasonable rate • Funding to local agencies to provide prenatal care has expanded their ability to serve women and children in need of prenatal and well child care
Impact of Reallocation of Funds • Utah PRAMS (Pregnancy Risk Assessment Monitoring System) – we started out with Title V funding as CDC did not have new funding • When new CDC money was available, we applied and now receive partial funding from CDC for the Utah PRAMS Project
Impact of Reallocation of Funds • Funding that previously served only 200 families per year now provides: • The opportunity for all Medicaid pregnant women to have better access to enhanced services, approximately 15,000 women per year • Prenatal care for more than 200 women per year in local clinics • Data for all mothers and newborns in the state (approximately 90,000 mothers and babies) to benefit from PRAMS DATA that is turned TO ACTION
How Title V Works in States • Funding decisions based on needs assessment and health systems needs • Utah determined that we needed more information on women who give birth so that we could work to improve the health of infants • If we put our allotment of Title V funding into prenatal care alone, we would not be able to cover the costs for all women in the state in need of prenatal care and we would not be able to identify the problems that are related to pregnancy and newborn outcomes
How Title V Works in States • So, why did we put Title V funds into PRAMS rather than services? • Oversight of Project is funded with Title V funds – personnel, etc. • DATA TO ACTION • We identified factors related to late or no prenatal care that we into a media campaign – 13 / 13
How Title V Works in States • “13 / 13” Campaign Media campaign designed to promote prenatal care starting before the 13th week and including 13 visits • TV spots • Lucky number • Mad scientist • Fortune teller • Radio spots • Currently evaluating the impact of the campaign
How Title V Works in States • We have identified factors related to prematurity that will help us understand the problem better • Provider education on infertility treatment standards • Education of women regarding the importance of planning for healthy pregnancies • Importance of previous pregnancy history
How Title V Works in States • We have identified factors related to the high percentage of women who experience moderate to severe depression during the months after the birth of their infant • Provider education on the importance of screening for depression • Public education on signs of depression
How Title V Works in States • We will soon publish analysis of PRAMS data that will provide information on obesity issues related to pregnancy • Provider education re counseling women before pregnancy regarding weight and possible impact on pregnancy outcomes • Public education re the importance of nutrition and physical activity to enhance health, including pregnancy outcomes
How Title V Works in States • By allocating the funding to work on health care system issues, barriers to care, etc. we are able to impact the system of care for more • Mothers reported that money was the primary reason for not getting into early prenatal care – so we embarked on the campaign that encouraged women to get in early, contact the Baby Your Baby Hotline to find out how they could get assistance with prenatal care and where they could go to get the care
Federally Required Fiscal Reporting • Source of funding – federal, state, private, etc. • Distribution among population served • Distribution by types of services