Download
1 / 14
210 likes | 917 Vues
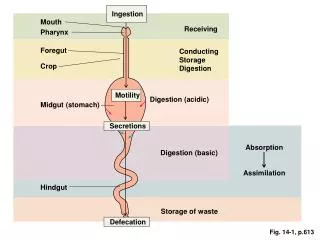
Small Intestine. Motility in the Small Intestine The functions of small intestinal motility are: 1. to mix foodstuffs with digestive secretions and enzymes, 2. circulation of contents to facilitate contact with mucosa for absorption,

E N D
Small Intestine Motility in the Small Intestine The functions of small intestinal motility are: 1. to mix foodstuffs with digestive secretions and enzymes, 2. circulation of contents to facilitate contact with mucosa for absorption, 3. net propulsion of luminal contents in the aboral direction. Following entry of nutrients into the small intestine, transit is initially rapid, to spread chyme along the small bowel. Transit then slows to promote absorption.
There Are 2 Major Types Of Small Intestinal Motility Peristalsis (“propulsion”) Segmentation (“mixing”) CONTRACTING SEGMENT RECEIVING SEGMENT
Propulsion In Small Intestine Also Involves A “Gradient Of Segmentation” 12 Segmentation rate (cycles/min) 10 8 80 160 240 Distance from incisors (cm)
Overview Of Intestinal Fluid Transport Maximal reabsorptive capacity of colon is approximately 5 L/day, Diarrhea > 5 L/day. Diet 2.0L Saliva 1.5L Gastric juice 2.0L Pancreatic juice 1.5L Bile 0.5L Small intestine 1L 6.5L small intestinal absorption 2.0L 1.9L colonic absorption stool water (100 ml approx.)
Small Intestine Is An Absorptive And A Secretory Epithelium absorption Surface tip maturation zone secretion crypt Base
Na+ Uptake Drives Fluid Absorption Via Several Different Pathways duodenum Na+ nutrient Na+ 3Na+ Cl- 2K+ Na+ H+ H2O Luminal membrane Basolateral membrane ileum
Why Would Intestinal Fluid Secretion Be Needed? • Aids lubrication and motility (secretion failure = gut obstruction) • Provides a source of Na+ to absorb nutrients if a meal has • low Na+ content • Vehicle for gut antibodies secreted from crypts General response to irritation/infection to “wash out” the problem
VIP Enterotoxin Enterotoxin Ach, 5-HT Cl- Transport Drives Fluid Secretion From Crypts cell cAMP lumen blood 2Cl- + K+ CFTR Na+ Cl- 3Na+ + 2K+ CACC Cl- Ca2+ Na+ and water Secretory Diarrhea
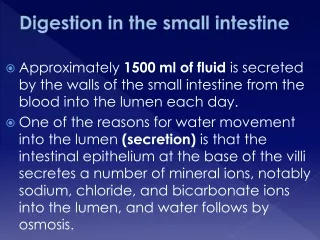
5. Secretions of the Small Intestine Brunner’s glands An extensive array of compound mucus glands Located in the wall of duodenum. Secrete mucus and HCO3- Crypts of Lieberkühn Located over the entire surface of the small intestine. Goblet cell: secrete mucus Enterocytes: secrete and absorb water and electrolytes
6. Secretions of the Large Intestine The large intestine has many crypts of Lieberkühn and secrets an alkline mucus solution containing bicarbonate and K+. The sole function of mucus is protection. It protects the large intestine wall from damage by acids formed in feces from attacking the intestinal wall. Acid and mechanical stimulation, mediated by both long and short reflexes, increase the secretion of mucus. the wall of the large intestine Acid passage of feces Neural reflexes (long and short) Mucus secretion a mucus layer lining the wall
Case: Zollinger-Ellison Syndrome Description of Case: A 52-year-old man visits his physician complaining of abdominal pain, nausea, loss of appetite, frequent belching, and diarrhea. The man reports that his pain is worse at night and is sometimes relieved by eating food or taking antacids containing HCO3-. GI endoscopy reveals an ulcer in the duodenal bulb. Stool samples are positive for blood and fat. His serum gastrin level is measured and found to be markedly elevated. A CT scan reveals a 1.5 cm mass in the head of the pancreas. The man is referred to a surgeon. While awaiting surgery, the man is treated with the drug omeprazole, which inhibits H+ secretion by gastric parietal cells. During a laparotomy, a pancreatic tumor is located and excised. After surgery, the man’s symptoms diminish, and subsequent endoscopy shows that the duodenal ulcer has healed. Explanation of Case: All of the man’s symptoms and clinical manifestations are caused, directly or indirectly, by a gastrin-secreting tumor of the pancreas. In Zollinger-Ellison syndrome, the tumor secretes large amounts of gastrin into the circulation. The target cell for gastrin is the gastric parietal cell, where it stimulates H+ secretion. The physiologic source of gastrin, the gastric G cells, are under negative feedback control. Thus, normally, gastrin secretion and H+ secretion are inhibited when the gastric contents are acidified (i.e., when no more H+ is needed). In Zollinger-Ellison syndrome, however, this negative feedback control mechanism does not operate: gastrin secretion by the tumor is not inhibited when the gastric contents are acidified. Therefore, gastrin secretion continues unabated, as does H+ secretion by the parietal cells.
Case: Zollinger-Ellison Syndrome, explanation (cont.) The man’s diarrhea is caused by the large volume of fluid delivered from the stomach (stimulated by gastrin) to the small intestine; the volume is so great that it overwhelms the capacity of the intestine to absorb it. The presence of fat in the stool (steatorrhea) is abnormal, since mechanisms in the small intestine normally ensure that dietary fat is completely absorbed. Steatorrhea is present in Zollinger-Ellison syndrome for two reasons. 1) The first reason is that excess H+ is delivered from the stomach to the small intestine and overwhelms the buffering ability of HCO3--containing pancreatic juices. The duodenal contents remain at acidic pH rather than being neutralized, and the acidic pH inactivates pancreatic lipase. When pancreatic lipase is inactivated, it cannot digest dietary triglycerides to monoglycerides and fatty acids. Undigested triglycerides are not absorbed by intestinal epithelial cells, and thus, they are excreted in the stool. 2) The second reason for steatorrhea is that the acidity of the duodenal contents damages the intestinal mucosa (evidenced by the duodenal ulcer) and reduces the microvillar surface area for absorption. Treatment: While the man is awaiting surgery to remove the gastrin-secreting tumor, he is treated with omeprazole, which directly blocks the H+-K+-ATPase in the apical membrane of gastric parietal cells. This ATPase is responsible for gastric H+ secretion. The drug is expected to reduce H+ secretion and decrease the H+ load to the duodenum. Later, the gastrin-secreting tumor is surgically removed.
Case: Resection of the Ileum Description of Case: A 36-year-old woman has 75% of her ileum resected following a perforation caused by severe Crohn’s disease (chronic inflammatory disease of the intestine). Her postsurgical management included monthly injections of vitamin B12. After surgery, she experienced diarrhea and noted oil droplets in her stool. Her physician prescribed the drug cholestyramine to control her diarrhea, but she continues to have steatorrhea. Explanation of Case: The woman’s severe Crohn’s disease caused an intestinal perforation, which necessitated a subtotal ileectomy, removal of the terminal portion of the small intestine. Consequences of removing the ileum include decreased recirculation of bile acids to the liver and decreased reabsorption of the intrinsic factor-vitamin B12 complex. In normal persons with an intact ileum, 95% of the bile acids secreted in bile are returned to the liver, via the enterohepatic circulation, rather than being excreted in feces. This recirculation decreases the demand on the liver for the synthesis of new bile acids. In a patient who has had an ileectomy, most of the secreted bile acids are lost in feces, increasing the demand for synthesis of new bile acids. The liver is unable to keep pace with the demand, causing a decrease in the total bile acid pool. Because the pool is decreased, inadequate quantities of bile acids are secreted into the small intestine, and both emulsification of dietary lipids for digestion and micelle formation for absorption of lipids are compromised. As a result, dietary lipids are excreted in feces, seen as oil droplets in the stool (steatorrhea). This patient has lost another important function of the ileum, the absorption of vitamin B12. Normally, the ileum is the site of absorption of the intrinsic factor-vitamin B12 complex. Intrinsic factor is secreted by gastric parietal cells, forms a stable complex with dietary vitamin B12, and the complex then is absorbed in the ileum. The patient cannot absorb vitamin B12 and must receive monthly injections, bypassing the intestinal absorptive pathway. The woman’s diarrhea is caused, in part, by high concentrations of bile acids in the lumen of the colon (because they are not recirculated). Bile acids stimulate cAMP-dependent Cl- secretion in colonic epithelial cells. When Cl- secretion is stimulated, Na+ and water follow Cl- into the lumen, producing a secretory diarrhea (sometimes called bile acid diarrhea). Treatment: The drug cholestyramine, used to treat bile acid diarrhea, binds bile acids in the colon. In bound form, the bile acids do not stimulate Cl- secretion or cause secretory diarrhea. However, the woman will continue to have steatorrhea.
Contraction of the gallbladder is correctly described by which of the following statements? a. It is inhibited by a fat-rich meal b. It is inhibited by the presence of amino acids in the duodenum c. It is stimulated by atropine d. It occurs in response to cholecystokinin e. It occurs simultaneously with the contraction of the sphincter of Oddi D.