Download
1 / 26
260 likes | 331 Vues
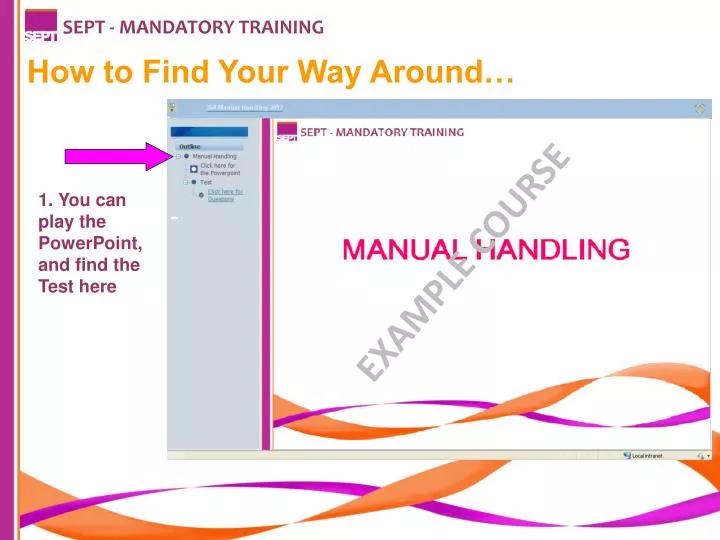
SEPT - MANDATORY TRAINING. How to Find Your Way Around…. 1. You can play the PowerPoint, and find the Test here. EXAMPLE COURSE. SEPT - MANDATORY TRAINING. 2. You can minimise this column and make the main page bigger by clicking this icon. Click it again to bring it back. EXAMPLE COURSE.

E N D
SEPT - MANDATORY TRAINING How to Find Your Way Around… 1. You can play the PowerPoint, and find the Test here EXAMPLE COURSE
SEPT - MANDATORY TRAINING 2. You can minimise this column and make the main page bigger by clicking this icon. Click it again to bring it back. EXAMPLE COURSE
SEPT - MANDATORY TRAINING 3. Always click this ‘Home’ icon to save your progress and log off. This is very important! EXAMPLE COURSE
SEPT - MANDATORY TRAINING NHS Protect ~ Security Management Background In April 2003, the NHS Security Management Service (SMS) was established, with a remit of encompassing policy and operation responsibility, for the management of security within the NHS; this included the protection of people, property and assets. In November 2003, the Secretary of State issued new national guidelines, regarding tackling violence against NHS staff. The aim of which was to deliver an environment that is safe and secure for staff, ensuring the highest standards of clinical care, are made available to patients. Subsequently a wide range of national guidance has been issued to NHS Trusts in relation to violence and security. The NHS Security Manual has also been provided to Trusts via access by the Local Security Management Specialist. In April 2011 the NHS Security Management Service was reviewed as part of a national review of government funded bodies and is now known as NHS Protect. COURSE OBJECTIVES • NHS Protect background • NHS Protect role • What security management means • The role of the Trust LSMS • Related Policies • Violence and aggression • De-escalation
SEPT - MANDATORY TRAINING The Role of NHS Protect NHS Protect has overall responsibility for all policy and operational matters, related to the management of Security within the NHS. NHS Protect leads on work to identify and tackle crime across the health service. The aim is to protect NHS staff and resources from activities that would otherwise undermine their effectiveness and their ability to meet the needs of patients and professionals. Ultimately, this helps to ensure the proper use of valuable NHS resources and a safer, more secure environment in which to deliver and receive care. • NHS Protect Structure • NHS Protect has been reorganised to have three distinct service areas: • Policy guidance for the NHS • 2. Deterrence of crime, violence and fraud in the NHS • 3. Operational security management and counter fraud services: • Local support and development services (to support LSMS’s and their NHS Trust) • National investigation services • Information and intelligence services • NHS Protect works closely with the Health & Safety Executive and the CQC in monitoring the required security management standards in NHS Trusts.
SEPT - MANDATORY TRAINING • The Local Security Management Specialist • As an organisation we have appointed an Accredited Local Security Management Specialist (LSMS), whose role is to implement the national security management strategy and guidance at SEPT. • Trained and accredited Local Security Management Specialists (LSMSs) have taken the lead in security management work in all health bodies since April 2004. • LSMS work takes place within a clear legal framework, set out in Directions issued by the Department of Health to relevant health bodies and the strategic framework outlined in the National Strategy document. • Only the LSMS may perform the duties and functions described in Directions, subsequent guidance and requirements specified in the NHS Security Management Manual. • The LSMS leads, assists in and co-ordinates the prevention strategies, investigation of all assaults and other criminal activity and resultant actions at SEPT. • The LSMS is the central contact point for NHS Protect, and will facilitate information sharing and gathering between SEPT and NHS Protect, including Safety Alerts and annual statistics relating to assaults within the organisation.
SEPT - MANDATORY TRAINING • The Local Security Management Specialist • The LSMS is the central contact point for the police and staff within SEPT when dealing with assaults and other criminal acts under investigation. • In addition to being SEPT's expert resource in matters of security management, the LSMS liaises with their Area Security Management Specialist, networks with their peers to maintain the ongoing development of their role. • Currently your LSMS's are Suzanne Deighton (for Mental Health & Learning DIsability Services) and Jo Englefield (for Community Health Services), who are based in the Risk Management Department in Essex. • Our Non-Executive Director, (NED) Steve Currell, ensures and monitors necessary requirements are in place within the Trust and guidelines adhered too. • The Director nominated as the 'Security Management Director' (SMD) is Peter Wadum- Buhl, Executive Director of Strategy & Business Development, who has overall responsibility for security management work with particular responsibilities for tackling violence within SEPT.
SEPT - MANDATORY TRAINING • NHS Protect Violence Strategy • NHS Protect is committed to tackling violence towards NHS staff. It strives to ensure strategies are developed and put in place to promote safer work environments for these staff. This is supported by Policy on Violence & Aggression at Work. • NHS Protect also recognises that staff working in certain settings have specific and complex needs. An example is mental health or learning disabilities settings, where there are higher levels of violence. Violence within these settings can be attributed to a range of factors, including environmental and cultural ones. • Secretary of State Directions state that all NHS front line staff must be trained in Conflict Resolution Training and in Mental Health & Learning Disability services a specific Promoting Safe & Therapeutic Services (PSTS), both are an integral part of the violence strategy and NHS Trusts are required to submit their training figures every year. • SEPT has incorporated this national guidance into its Prevention & Management of Violence & Aggression (PMVA) Policy and Procedural Guidelines (RM05) and provides a range of PMVA training based on staff role.
SEPT - MANDATORY TRAINING Property & Assets • NHS Protect works to protect and secure NHS property and assets. • In the document A Professional Approach to Managing Security in the NHS, property is defined as ‘the physical buildings in which NHS staff and professionals work, where patients are treated and from where the business of the NHS is delivered’. • In the same document, assets are defined as ‘the materials and equipment used to deliver NHS healthcare. In respect of staff, professionals and patients it can also mean the personal possessions they retain whilst working in, using or providing services to the NHS’. • These definitions also cover assets donated to or acquired by the health bodies, as these allow NHS staff and professionals to deliver healthcare to patients.
SEPT - MANDATORY TRAINING Property & Assets NHS Protect is undertaking work in the following areas: • ensuring the security of all NHS property and assets, regardless of type, size or value; • joint work with the Home Office to make all NHS car parks safe; • providing guidance on security in NHS maternity and paediatric units; • Secure by Design – work to explore ways in which security can be ‘designed in’ at planning stage for new builds and refurbishment in the NHS. • Lockdown Guidance and training to enable Trusts to deliver robust Lockdown policies, procedures and local plans.
SEPT - MANDATORY TRAINING • Counter Terrorism • In response to the terrorist threat, NHS Protect is committed to working with national, regional and local stakeholders to ensure that all Trusts identify vulnerability and adopt risk-assessed proportionate protective security measures. • NHS Protect provides guidance and support to LSMS's to deliver the 'Protect' strand of 'Contest' - which is the Governments national counter - terrorism strategy: • CONTEST is organised around four principal workstreams: • Pursue: to stop terrorist attacks • Prevent: to stop people from becoming terrorists or supporting terrorism • Protect: to strengthen our protection against terrorist attack • Prepare: where an attack cannot be stopped, to mitigate its impact • SEPT has policies for Management of Security (RM09) and specific guidance for managing a Bomb Threat or Hoax (Appendix RMPG09b)
SEPT - MANDATORY TRAINING • NHS Protect Legal Protection Unit (LPU) • The NHS Protect Legal Protection Unit (LPU) works closely with the following bodies to safeguard NHS staff and assets from violent and disruptive individuals: • the police • the Crown Prosecution Service • local authorities • health bodies. • It does this by providing advice and assistance on a wide variety of issues and, in appropriate cases, commencing legal proceedings. The LPU can take action in the civil courts to obtain injunctions, and can also seek antisocial behaviour orders. • Where appropriate, the LPU, in conjunction with NHS Trusts, will prosecute individuals who have assaulted or abused NHS staff, in cases that have not been progressed by the police or the Crown Prosecution Service. This approach has led to the successful prosecution of a number of individuals who would otherwise have escaped justice.
SEPT - MANDATORY TRAINING • NHS Protect Legal Protection Unit (LPU) • The LPU assists NHS Trusts with: • legal advice on issues such as withholding treatment • legal advice on the most appropriate sanctions available for specific cases • legal advice on the most appropriate redress available for specific cases • legal advice in cases of physical and non-physical assault • drafting warning letters and acknowledgement of responsibilities agreements. • The LPU also works proactively, contributing to the numerous official consultation processes that feed into national initiatives and policies. It works closely with the NHS Protect's policy team to develop policy guidance on issues such as confiscating weapons on NHS premises. • Members of the LPU write and update large parts of the NHS Security Manual (only available to Accredited Security Management Specialists).
SEPT - MANDATORY TRAINING • Area Security Management Specialist's • NHS Protect employs regional Area Security Management Specialists who provide operational support to the network of Local Security Management Specialists. • Area Security Management Specialists (ASMSs) provide the link between the network of Local Security Management Specialists and NHS Protect, ensuring that operational work informs and drives revision of national policy, systems and procedures. • The ASMS’s manage the regional Local Security Management Specialist networks, ensuring that best practice is highlighted and that updated legal and procedural information is made available.
SEPT - MANDATORY TRAINING • Security at SEPT • SEPT has a legal responsibility to provide a safe and secure environment for staff, service users and visitors. • SEPT employees also have a responsibility to ensure that both their personal property and Trust property and assets they have access to are managed securely. • All security related incidents must be reported on Datix. If you identify any security risks or issues, you must discuss with your line manager and/or contact the LSMS for advice. • There is a comprehensive Management of Security Policy and Procedural Guideline in the policy library (RM09) which can be found in the Risk Management Policy Folder here: http://tchw2kent02/documents.php?doc_id=9821 • All staff are expected to comply with this policy and guideline at all times
SEPT - MANDATORY TRAINING Lone working NHS Protect defines lone working as: 'any situation or location in which someone works without a colleague nearby; or when someone is working out of sight or earshot of another colleague‘ The Health and Safety Executive (HSE) defines lone workers as: 'those who work by themselves without close or direct supervision' A Lone Worker is a member of Trust staff who works, either regularly or only occasionally, on their own, and without access to immediate support from managers or other colleagues. This could be outside of a hospital or similar environment or internally. Lone Working may be a part of a person’s usual role or it could occur on an infrequent basis. Lone Working is not unique to any particular groups of staff, working environment or time of day. There is not one single definition that encompasses all those who may face lone working situations and, therefore, may face increased risks to their security and safety. All lone worker staff must have a risk assessment undertaken by their line manager to ensure that suitable and sufficient control measures are in place The Trust Lone Worker Policy & Procedural Guidelines (CLP38) can be found here: http://tchw2kent02/documents.php?doc_id=10238 The LSMS manages the NHS Lone Worker Service (lone worker devices) at SEPT.
SEPT - MANDATORY TRAINING Definitions of Violence The HSE (1997) describe physical assault and non-physical assault as: Physical Assault - The intentional application of force to the person or another, without lawful justification, resulting in physical injury or personal discomfort. Non-physical Assault - The use of inappropriate words or behaviour causing distress and / or constituting harassment. • The Public Health Model • This model is advocated by the World Health Organisation as the cornerstone of attempts to address workplace violence views prevention as having three dimensions. Each dimension is important but the emphasis is on primary prevention. • The model is shown below: • Primary prevention - preventing violence before it happened by addressing root causes • Secondary prevention - reactive responses de-escalation • Tertiary prevention - physical interventions post incident reviews and debriefs • Prevention at every level of the model requires: • Action at the level of the organisation • The staff team • The individual worker • The service user Violence & Aggression Model Bailey (1997) felt that for violence to take place, all 4 of the elements mentioned below must be present. The removal of any one of the above will result in a reduction in the risk of violence, in the same way as fire, heat, fuel and oxygen are all necessary for a fire, and removal or absence of any of the four will end a fire. Adapted from Bailey 1977 in Paterson B, Leadbetter D & McCornish A. "De-escalation in the management of aggression and violence." Nursing Times September 3, Volume 93, No 36 (1997)
SEPT - MANDATORY TRAINING First Line Intervention To de-escalate a developing situation, verbally is clinically ethically and legally preferable to using physical restraint. De-escalatory procedures should therefore be utilised in any arena that requires workers to come into contact with a potentially violent individual. Triggers, Weapons & Targets Triggers Triggers of violence and aggression are: Verbal - phrases which evoke anger / frustration; Physical - causing pain / discomfort, touch, invading personal space, poor use of body language; Environmental - noisy surroundings, lack of privacy, peer pressure towards anti-social behaviours. The above may sometimes involve causing offence to an individual on the grounds of their sexuality, culture of spiritual beliefs, or just unluckily pressing the wrong button(s). Weapons Some body parts may be used as a weapon, where inanimate objects are concerned. Targets The recipient of the assailant's aggression. • Circles of Influence • This concept is relatively simple. There are certain things that we have significant control over, notably our own non-verbal and verbal behaviour. There are other factors that are role dependant, which we may have less control over, such as the behaviour of other members of staff (although there is a responsibility to report abuse). • Commonly reported reactions to violence and fear and / or frustration and anger. Unless all three are acknowledged and managed, it can: • Diminish cognitive control • Evoke your own fight or flight reaction • Promote a desire to punish the service user for making us feel like this
SEPT - MANDATORY TRAINING Counter Aggression Counter aggression, in a care setting, is inappropriate. At times an assertive response may be necessary and warranted, but not an aggressive one. Staff have a responsibility to recognise and manage their own emotions and monitor the emotions of other staff, involved in a situation, to ensure safety of all • Managing your Emotions • Recognise and acknowledge signs of anxiety; • Recognise danger signals of your own and others' anger; • Take one deeper, than normal, breath and exhale slowly; • Use positive self statements (e.g. I can cope); • Focus on active listening; • Avoid a defend-attack spiral; • Choose what you are going to do • Violent Incident Models • There are five possible incident models; the underlying idea is that each incident is a unique event. However there may be common patterns amongst types of incidents. If staff can learn to recognise incident types, then they can adapt their response accordingly. • The five possibilities are: • Affective • Instrumental • Mixed • Aversive • Stimulus - Response – Consequence
SEPT - MANDATORY TRAINING Non-verbal De-escalation Verbal de-escalation is a skilled intervention, that is specifically used to intervene, when a patient's behaviour moves from being normal, for that individual, to a state that can be recognised as pre-aggressive. The technique particularly lends itself to use by health care workers, who spend long periods of time with patients, have formed a relationship and can note the early warning. It is important to appreciate and attend to our and others non-verbal behaviours and the need for cultural sensitivity. For example, in Iranian communities, thumbs-up, which indicates good in many western societies, is generally considered very rude. Any response to a potential incident must be guided in the first instance with an awareness of the risk the situation presents. The options are to stay or to leave the situation.
SEPT - MANDATORY TRAINING PERFECT Having decided that it is safe to stay, it is suggested that the acronym PERFECT is used to summarise aspects of practice. Proxemics (stance / posture / space) - Angry and aroused people have an increased need for personal space. Staff can therefore provoke incidents unwittingly by not respecting this need for increased distance or by adopting a confrontational posture. It is best to avoid standing directly in front of a service user who is angry. A stance that places the member of staff at an angle of about 45 degrees to the service user, whether sitting or standing, should be adopted. Eye Contact - Eye contact should try to remain akin to that of a normal conversation. Prolonged direct eye contact where the service user is highly aroused should be avoided as it can be interpreted provocatively. Avoidance of eye contact may be interpreted as submissive or fearful. Respect Touch Boundaries - The use of touch when someone is highly aroused requires extreme care. It must always be done in a way that respects dignity and individuality of service users. If the service user is angry, touching should be avoided altogether or done very slowly, so that the reaction can be observed and preferably with the service users explicit permission. Facial Expression - Facial expression is important as it serves to convey and reinforce the context of speech. Facial expression should ideally remain neutral; smiling should be avoided as it can be interpreted as laughing at the person.
SEPT - MANDATORY TRAINING Environment - The environment has both physical and social dimensions. Incidents can occur in front of an audience of other service users and staff. This influence must be judged; it could be a positive influence in this case the environment should remain unaltered. At other times it can exacerbate the situation making it harder for involved parties to negotiate. In this circumstance a change of environment should be considered. Consider Influence of your Appearance - Appearance forms part of the dynamic. A smart suit may convey one message whilst unshaven or chipped nail varnish another. Appearance is generally not right or wrong, however clothing that may be perceived as overly sexual is inappropriate in professional settings. Think about your Hand Movements - Palms should be open in view of the service user and not in pockets, arms folded, or hands on hips, which may be viewed as aggressive. This stance already described and posture demonstrates minimum treat to the service user but is not submissive. In addition if forms the basis for the defensive posture should violence occur. In addition to the above, active listening should also be utilised where appropriate. Active listening refers, not just to being attentive to what the person is saying and picking up on all relevant topics, but also refers to appearing to be paying attention. A client talking to someone who appears disinterested may very quickly become frustrated. Nodding, having your face directed towards the client, saying yes, right, etc are all useful responses to the client. Another useful skill, utilised in active listening, is where some of what the client has said is rephrased or repeated.
SEPT - MANDATORY TRAINING Verbal Skills Verbal communication is of equal importance to non-verbal. There are five aspects to consider that form the acronym LOADS. Learn to Manage Pitch / Tone / Volume - Pitch tone and volume are integral to communication and close attention is warranted. The aim of speech is to convey an empathic response and avoid escalating the situation further. Do not rush into a situation imagining that you know what is going on. Getting it wrong may cause further upset. Much better to ask the client what is bothering him / her, so that they can tell you what the issues are. Asking questions such as: are you okay? What is upsetting you? what can I do to help / sort this out? Not only does this provide you with information, so that you can work on info provided. It also gives the client the chance to ventilate, verbally what otherwise may only release through physical means. Overload with Agreement - Where the service user is extremely angry / distressed suggestions are that staff should consider agreeing with everything they say. The goal of this is to avoid giving the person a reason to escalate from verbal to physical violence. Where anger is less extreme, consider the idea of partial agreement.
SEPT - MANDATORY TRAINING Acknowledge and Check Feelings - Acknowledging feelings is an important dimension of practice. In the context of de-escalation, where the incident appears affective, the person is visibly aroused, red or white in the face, then an acknowledgement might be helpful. In situations where affective arousal appears missing, it can be helpful to acknowledge your own feelings to prompt the service user to reflect on their own behaviour. Empathy can be an affective tool, so try to imagine: how you would feel in their situation; what you would want, feel you need; how you would want to be treated. These considerations should not only assist us in choosing our approach, but if the client sees that you're trying to see things how he / she sees them, then this may build a better rapport based on mutual respect. Distraction - If the source of the anger is something that is outside your control, then a suitable strategy may be to move from the irresolvable conflict to a different compromise that can be attained. Temporary distraction can sometimes be managed by offer to phone, write or make tea. When the person is very angry, asking detailed questions, which requires the person to think, engages recall, which can prompt the re-engagement of cognitive control. It is sometimes tempting to make promises, but caution should be exercised if they cannot be fulfilled. Start Negotiations - Negotiation has a series of discreet stages starting with establishing and agreement to negotiate. Certain things may not be negotiable, so it is helpful to clarify what is and what is not negotiable. Ground rules for negotiation can include no shouting or swearing, exemplified by limit setting (e.g. 'I am here to listen to you, but I need you to sit down and stop swearing before we do that').
SEPT - MANDATORY TRAINING Accepting When We Are in the Wrong Sometimes we accept that the client is right, and for whatever reason, they have been treated badly or wronged. Though some will still bear a grudge, most people will accept to some extent, an apology. It is easy if you are a person in a position of authority to wield your power proudly. Sometimes all that is required in an aggressive situation is to admit you or your service, were wrong or failed the client. For example, "I'm sorry, sometimes I talk without thinking, I didn't mean that, the way it came out" or "I'm sorry, I know you've been told just five minutes, too may times, you should have been seen by now and I apologise." De-escalation Caveats De-escalation is not treatment. Where aggressive or violent behaviour can be foreseen, planned de-escalation strategies must be part of a behaviour management plan, which in turn must be part of behavioural change strategies. Contact Details To contact your Local Security Management Specialist and Risk Department
SEPT - MANDATORY TRAINING Now You need to take the Test. Please click the ‘Test’ icon in the left column, and then click for Questions. Remember to click the ‘Home’ icon when you finish the Test to save your results EXAMPLE COURSE