Download
1 / 36
460 likes | 945 Vues
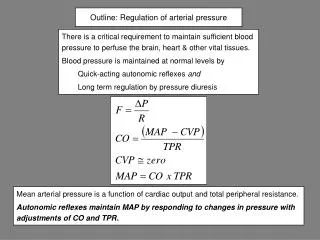
Long Term Regulation of Arterial Blood Pressure and Hypertension. Balance Between Fluid Intake and Output. Pressure Natriuresis . Arterial pressure is a signal for regulation of NaCl excretion.

E N D
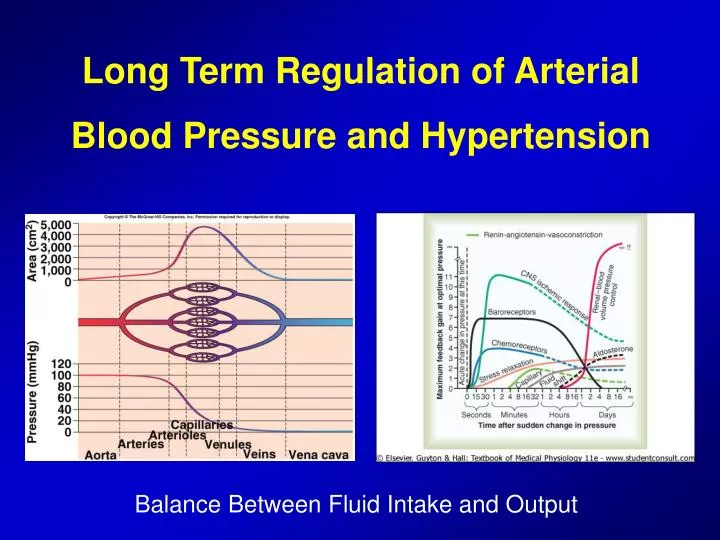
Long Term Regulation of Arterial Blood Pressure and Hypertension Balance Between Fluid Intake and Output
Pressure Natriuresis.Arterial pressure is a signal for regulation of NaCl excretion. • arterial pressure NaCl reabsorbed in the proximal tubule more NaCl to the macula densa TGF autoregulation RBF, GFR. • Pressure natriuresis can normalize BP by decreasing the effective circulating volume – this response connects BP and ECFV.
Renal-Body Fluid System for Arterial Pressure Control • When the body contains too much extracellular fluid, the blood volume and arterial pressure rise • Pressure Diuresis and Pressure Natriuresis • At high pressure, the kidneys excretes the excess volume into urine and relieves the pressure • At low pressure, the kidney excretes far less fluid than is ingested
Renal Urinary Output Curve or Renal function curve
Pressure Control by Renal-Body Fluid Mechanism • Over the long period, water and salt output must equal intake • Equlibrium point • Return of the arterial pressure always exactly back to the equlibrium point in the “infinite feedback gain” principle
Two Determinants of Long-Term Arterial Pressure Level • The degree of pressure shift of the renal output curve for water and salt • The level of water and salt intake line • It is impossible to change the long-term mAP level to a new value without changing one or both of the two basic determinants of long-term AP
Failure of increased TPR to elevate the long-term level of AP if fluid intake and renal function do not change • AP = Cardiac output x Total Peripheral Resistance • So, increase in TPR should elevate AP • But this acute rise in AP is not maintained if the kidneys function properly • Why? • Pressure diuresis and pressure natriuresis
Failure of increased TPR to elevate the long-term level of AP if fluid intake and renal function do not change
Increased Fluid Volume Can Elevate AP by Increasing Cardiac Output or Total Peripheral Resistance
Importance of salt (NaCl) in the renal-body fluid diagram for arterial pressure regulation • An increase in salt is far more likely to elevate AP than is an increase in water intake • Water can be eliminated easily, but salt not • Accummulation of salt in the body • Stimulation of thirst center in the brain • Increased osmotic pressure stimulates release of vasopressin (ADH)
Hypertension “Hypertensionis defined as sustained abnormal elevation of the arterial blood pressure”
Hypertension • Leads to wear and tear • is a major risk factor for cardiovascular diseases such as: • STROKE • HEART FAILURE • ATHEROSCLEROSIS 30% of world’s deaths
Complications Complications as a result of hypertension include: Stroke Dementia Myocardial Infarction Congestive Heart Failure Retinal Vasculopathy Renal Disease or Failure
Chronic Hypertension is Caused by Impaired Renal Function • Mean Arterial Pressure > 110 mmHg (normal is about 90 mmHg) • Systolic >140, diastolic >90 mmHg • Hypertension can be lethal • Heart failure • Damage of a large vessel in the brain (cerebral infarct or stroke) • Kidney failure • Volume-loading hypertension means hypertension caused by excess accumulation of extracellular fluid in the body
Volume-loading hypertension • Reduced renal mass and increased salt intake
Volume-loading hypertension: Two separate sequential stages • The first stage: increased fluid volume causing increased cardiac output hypertension • The second stage: High blood pressure, high TPR but return of the cardiac output near the normal • Hypertension • Marked increase in TPR • Almost complete return of the extracellular fluid volume blood volume and cardiac output back to normal Volume-loading hypertension in patients who have no kidneys and need for dialysis
Hypertension caused by primary Aldosteronism • Another type of volume-loading hypertension is caused by excess aldosterone in the body – (other steroids) • A small tumor of adrenal glands and primary aldosteronism • Aldesteron increases reabsorbtion of salt and water increased blood volume and reduced urine output • Consequently, hypertension develops
The Renin-Angiotensin SystemPressure control and Hypertension • Renin is an enzyme released by the kidneys when the arterial pressure falls too low • It is synthesized and stored in inactive form called prorenin in juxtaglomerular cells • JG cells are modified smooth muscle cells in the walls of afferent arterioles • Renin acts on angiotensinogen (a plasma globulin) • Half life of renin is about 30 mins • Angiotensin I, converting enzyme and Angiotensin II
The Renin-Angiotensin SystemPressure control and Hypertension
Rapidity and Intensity of Vasoconstrictor Pressure Response to the Renin-Angiotensin System • Renin-angiotensin vasoconstrictor system requires about 20 mins to become fully active
Effect of Angiotensin in the Kidneys to Cause Renal Retention of Salt and Water • Angiotensin acts directly on the kidneys to cause salt and water retention • Makes the kidneys retain salt and water • Causes vasoconstriction in renal arteries • Angiotensin causes the adrenal gland to secrete aldosterone - Aldosterone increases salt and water retention by the kidneys
Role of Renin-Angiotensin System in Maintaining a Normal Arterial Pressure Despite Wide Variations in Salt Intake • When the renin-angiotensin system functions normally, pressure rises no more than 4 to 6 mmHg in response to as much as a 50-fold increase in salt intake
Other Types of Hypertension Caused by Combinations of Volume-Loading and Vasoconstriction • Aort Coarctation – hypertension • High BP in the upper body, but BP is normal in the lower body • Autoregulation of hypertension
Coarctation of the Aorta • Coarctation usually occurs just distal to the left subclavian artery at the ligamentum arteriosum • May also occur just proximal to the left subclavian. • Causes systemic hypertension and secondary LVH with heart failure.
Other Types of Hypertension Caused by Combinations of Volume-Loading and Vasoconstriction • Hypertension in pre-eclampsia (toxemia of pregnancy) • Ischemia of the placenta and subsequent release of toxic factors causing hypertension • Endothelial dysfunction – reduction of Nitric Oxide • Impaired renal pressure natriuresis • Development of hypertension • Thickening of the kidney glomerular membranes (auotoimmune process)
Other Types of Hypertension Caused by Combinations of Volume-Loading and Vasoconstriction • Neurogenic Hypertension • Acute neurogenic hypertension can be caused by strong stimulation of the sympathetic nervous system • Excitement, anxiety induces sympathetic activity which causes peripheral vasoconstriction and acute hypertension occurs • Acute neurogenic hypertension caused by sectioning the baroreceptor nerves
Primary (Essential) Hypertension • 90 to 95% of hypertension cases are of primary • It is of unknown origin • Genetics: there is a strong hereditary tendency • Environment: Excess weight and sedentary life style • Neurohormonal mediators
Some Characteristics of Primary Hypertension • Cardiac output is increased due to additional blood flow required for the extra adipose tissue and increased metabolism • Sympathetic nerve activity (especially in kidneys) is increased in OW patients (leptin – vasomotor center ?) • Angiotensin II and aldosterone are increased (sympathetic stimulation-renin-aldosterone …) • Renal-pressure natriuresis mechanism is impaired • If hypertension is not treated, there may also be vascular damage in the kidney that can reduce glomerular filtration rate
Graphical Analyses of AP Controling Primary Hypertension Reason for the difference between non-salt and salt-sensitive hypertension is probably related to structural and functional differences in kidney (nephrons..)
Treatment of Primary Hypertension • Two general classes of drugs are used • Vasodilator drugs that increase renal blood flow • Natriuretic and diuretic drugs that decrease tubular reabsorption of Na and water • Vasodilator drugs • Inhibiting sympathetic nerve activity to kidneys • Direct relaxation of smooth muscle of renal vasculature • Blocking the action of renin-angiotensin system on renal vasculature or tubules
Summary for Arterial Pressure Regulation • AP is regulated not by a single pressure controlling system (several inter-related systems) • To achieve • Survival • Returning the blood volume and pressure back to normal • Mechanisms • Rapidly acting pressure control mechanisms • Intermediate mechanisms that act after several minutes – hours • Long-term arterial pressure regulation
Intermediate mechanisms that act after several minutes – hours • Renin-Angiotensin vasoconstrictor mechanism • Stress-relaxation of the vasculature • Shift of fluid through capillary walls in and out of circulation * These mechanisms become mostly activated within 30 mins to several hours
Long term mechanisms for AP regulation • Role of the kidneys • Many factors can affect pressure-regulating level of the renal-body fluid mechanism • Aldosterone • Renin-Angiotensin system • Nervous system (increased sympathetic activity)