Download
1 / 13
130 likes | 226 Vues
Autoimmune thyroid disease: old and new players. DeMarco, V. G. et al. Nat. Rev. Endocrinol. 10, 364–376 (2014). Introduction.

E N D
Autoimmune thyroid disease: old and new players DeMarco, V. G. et al. Nat. Rev. Endocrinol. 10, 364–376 (2014)
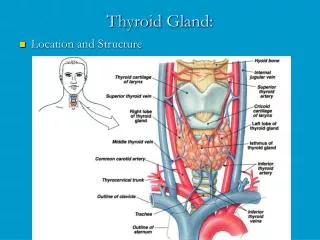
Introduction • Autoimmune thyroid disease (AITD) is a multifactorial or so-called ‘complex’ disease in which autoimmunity against thyroid antigens develops against a particular genetic background facilitated by exposure to environmental factors • AITD encompasses a spectrum of conditions ranging from Hashimoto’s hypothyroidism (HH) at one end to Graves’ hyperthyroidism (GH) at the other end • Thyroid peroxidase (TPO) and thyroglobulin (Tg) are the major autoantigens in Hashimoto’s disease, but TPO-Ab and Tg-Ab occur also in ~70% of patients with Graves’ disease
Introduction This review focuses on what has been learnt in the last 10 years on the etiology of AITD: • Is the predilection for female gender better understood? • Have new susceptibility genes been detected? And has progress been made with respect to environmental insults? • Have there been new players in this field, or have remaining issues with old players been clarified? • Finally, if individuals are at risk to develop AITD in view of their family history of AITD, is there anything they can do in terms of AITD prevention?
Existential factors: Parity • Parity as a risk factor for AITD has received much attention in relation to fetal microchimerism • There is transfer of fetal cells into the maternal circulation, already in the first trimester • Fetal microchimerism results when fetal cells persist in maternal tissues, and it is hypothesized that maternal immune responses against foreign fetal antigens might trigger autoimmune diseases • Fetal microchimerism has indeed been found in blood and thyroid tissue from women with Hashimoto’s or Graves’ disease
Existential factors: Parity • Using parity as a surrogate for increasing fetal cell exposure, one would expect the higher the number of pregnancies is, the higher the frequency and/or concentration of thyroid antibodies will be • However, the results have been conflicting • Several population-based studies have observed that there was no association between parity and TPO-Ab any longer after adjustment for maternal age and other important confounders • Other equally large studies do report associations that remain significant after adjustments, using higher cutoff values for TPO-Ab positivity
Existential factors: X-chromosome inactivation • A skewed X-chromosome inactivation (XCI) is defined – arbitrarily – as inactivation of the same X chromosome in ≥80% of cells • The consequence could be that self-antigens on one X chromosome are not expressed at sufficiently high levels in the thymus or at peripheral sites involved in tolerance induction • Loss of immunological tolerance to X-linked antigens might induce autoimmunity • The epigenetic phenomenon of skewed XCI may, in part, explain the strong female preponderance in AITD
Genetic factors • Single-nucleotide polymorphisms (SNPs) in TSHR have been specifically associated with Graves’ disease and not with autoimmune hypothyroidism in a Caucasian population • The functional consequences of these intronic SNPs are not entirely clear • They could give rise to RNA splice variants, increasing the level of potential autoantigenic TSHR-A subunits • Alternatively, SNP carriers may have fewer thymic TSHR mRNA transcripts, which may decrease central tolerance to TSHR
Genetic factors • The immunoregulatory genes HLA class II, CTLA4, and PTPN22 were already recognized as risk factors in the 20th century by case–control studies • They are all involved in the immunological synapse, in which antigenic peptides complexed in HLA molecules are presented by antigen-presenting cells to T-cell receptors on T-cells • Polymorphisms in these genes are not specific for AITD, as they also confer susceptibility for other autoimmune diseases
Environmental factors: New players • Smoking is a well-established risk factor for Graves’ disease • The OR for GH is 3.30 (95% CI, 2.09–5.22) in current smokers when compared with never smokers • The OR for Graves’ ophthalmopathy is even higher: OR 4.40 (95% CI, 2.88–6.73) in ever smokers vs never smokers • In the last few years, however, convincing evidence has been obtained that current smoking protects against (autoimmune) hypothyroidism • Although smoking is an old player in the relation between environmental exposures and autoimmunity, the discovery of its protective effect allows the label ‘new player’
Environmental factors: New players • Alcohol is known to protect against other autoimmune diseases such as rheumatoid arthritis and type 1 diabetes • However, the effect of alcohol on the immune system is complex, and how alcohol suppresses autoimmunity remains incompletely understood • A Cochrane systematic review concludes that data at present do not allow confident decision making about the use of selenium supplementation for Hashimoto’s thyroiditis • Low vitamin D levels have been identified as a risk factor for various autoimmune diseases such as type 1 diabetes, rheumatoid arthritis, multiple sclerosis, & Crohn’s disease. The situation with respect to AITD is less clear
Environmental factors: Old players • Thyroid antibodies and autoimmune hypothyroidism are more common in iodine-replete areas than in iodine-deficient areas • Further elegant proof of this has recently been obtained from population-based studies in Denmark • Prevalence figures before and after mandatory iodization of salt were 14.3 and 23.8% for TPO-Ab, and 13.7 and 19.9% for Tg-Ab respectively; ORs were 1.80 (TPO-Ab) and 1.49 (Tg-Ab) • In contrast to Graves’ disease, stress is apparently not involved in Hashimoto’s thyroiditis
Possible preventive interventions to decrease risk of developing autoimmune thyroid disease