Download
1 / 106
1.06k likes | 1.26k Vues
Nutritional Anemias. Spenser Parker, Katie Gardner, Juliette Soelberg , McKell Compton. Case Study. Patient SH 31 yr. old female 23 rd week of gestation, 3 rd pregnancy Chief complaint:

E N D
Nutritional Anemias Spenser Parker, Katie Gardner, Juliette Soelberg, McKell Compton
Case Study • Patient SH • 31 yr. old female • 23rd week of gestation, 3rd pregnancy • Chief complaint: • Fell on ice and has had abdominal pain and vaginal spotting. Questioned if she was beginning premature labor • Dx: microcytic, hypochromic anemia 2o to iron deficiency • Discharged the following day on 40 mg ferrous sulfate TID
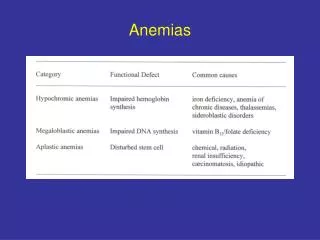
Basic terms • Anemia: a deficiency in the size or number of RBC or the amount of Hgb they contain that limits the exchange of oxygen and carbon dioxide • Macrocytic: larger-than-normal RBC • Microcytic: smaller-than-normal RBC • Megaloblastic: large, immature, abnormal, RBC • Hypochromic: deficient Hgb content and pale color of RBC • Normochromic: sufficient Hgb content of RBC • CBC: complete blood count
CBC • Includes: • Total blood cell (TBC) count • Hemoglobin • Hematocrit • RBC indices (measurements of the volume, size, distribution and Hgb content of RBC) • WBC count and differential count • Blood smear • Platelet count and mean platelet volume (MPV)
Occurs in bone marrow • Erythrocytes derived from precursor cells, erythroblasts/ normoblasts • Abnormal erythroblasts called megaloblasts • Erythropoietin stimulates uncommitted stem cells to differentiate into proerythroblasts • Hgbis apparent and increases in quantity as nuclear size shrinks • Reticulocyte matures into an erythrocyte within 24 to 48 hours • Erythrocyte loses its capacity for Hgb synthesis and oxidative metabolism Erythropoiesis
Hemoglobin Synthesis • Hgb: the substance that reversibly binds oxygen • Each hemoglobin molecule consists of two parts • 1. a protein “globin” part, composed of four polypeptide chains • 2. Four disk-shaped pigment molecules called “hemes”. Each heme has an iron molecule in the center. Fe++(ferrous iron) + porphyrin= Heme • Each heme molecule is capable of carrying one molecule of oxygen • Ferric iron carries an extra positive charge and forms methemoglobin, forming an unstable type of hgb not capable of binding oxygen
Iron • Adult body contains 2 major pools of iron • 1. functional iron in hgb, myoglobin, and enzymes • 2. storage iron in ferritin, hemosiderin, and transferrin (transport protein in blood) • Iron is highly conserved by the body • 90% is recovered and reused everyday • The rest is excreted mainly in the bile • Dietary iron must meet this 10% gap to maintain iron balance or else iron deficiency result • Dietary iron exists in two chemical forms: heme and nonheme
Heme Iron • Heme iron: in hemoglobin, myoglobin, and some enzymes from animal sources • absorbed across brush border after digested from animal sources. • the ferrous iron is enzymatically removed from the ferroporphyrin complex • the free iron ions combine with apoferritin to form ferritin • iron stores are moved into blood at the basolateral membrane involving an active transport mechanism
Nonheme Iron • Nonheme iron: mainly in plant foods but also in some animal foods • must be in a soluble (ionized) form to be transferred across the brush border • acid of gastric secretions enhance the solubility and change the iron to the ionic state either as ferric (+3) or ferrous (+2) oxidation state • divalent metal transporter 1 (DMT1) transports ferrous iron across the border • the ferrous (+2) form is absorbed more readily, ferric iron (+3) has to be reduced by ferric reductase to be absorbed • the ferrous iron is then bound to apoferritin and goes through the same process as with heme iron to enter the blood
Absorption • Efficiency of absorption is controlled by intestinal mucosa allowing certain amounts of iron to enter blood from the ferritin pool according to the body’s needs • Hepcidin produced by liver acts on mucosa cells and inhibits absorption of iron. • Another signal from body to the absorbing cells may be transferrin saturation. • A low %TIBC of transferrin would stimulate absorbing cells to transport iron across the basolateral membrane to the blood. If iron concentration is excessive, absorbing cells would be down regulated and less iron would be absorbed • When circulating % transferrin saturation is low, the new intestinal cells (intestinal cells are sloughed off every 5 to 6 days) will have more receptors for iron absorption
Iron Deficiency Anemia • World’s most common nutritional deficiency disease • Iron deficiency results in decreased production of hemoglobin (Hgb) • Which in turn results in microcytic, hypochromic anemia • This anemia is the last stage of iron deficiency, representing a long period of iron deprivation
Etiology • Inadequate ingestion • Inadequate absorption • Inadequate utilization • Increased requirement • Increased blood loss or excretion • Defects in release from stores
Inadequate Absorption • Medications that cause GI bleeding (aspirin, NSAIDS) • Diarrhea (decreases intestinal transit time/absorption) • Achlorydria (production of gastric acid is not present or low) • Celiac disease • Atrophic gastritis • Partial or total gastrectomy • Drug interference (antacids, cholestyramine, cimedtidine [Tagamet], pancreatin, ranitidine [Zantac], tetrcycline, and antiretroviral medications [especially the necleoside reverse transcriptase inhibitors, Combivir, Epivir, Retrovir, Zerit and the protease inhibitor Crixivan])
Stages of Deficiency • Stages of negative iron balance • I: Moderate depletion of iron stores; no dysfunction • II: Severe depletion of iron stores; no dysfunction • III: Iron deficiency; dysfunction • IV: Iron deficiency; dysfunction and anemia
Measurements Of Iron Deficiency • Plasma ferritin • Plasma iron • Total circulating transferrin • Saturation of circulating transferrin • Saturation of ferritin with iron • Soluble serum transferrin receptor (STFR)
Diagnosis • Diagnosis requires more than one method of iron evaluation • Preferably the first three measurements • Should also include an assessment of cell morphology • Serum or plasma ferritin level is the most sensitive parameter of negative iron balance (decreases only in presence of true iron deficiency, as with transferrin saturation)
Laboratory Tests • Normal Levels: • Ferritin: Males:12-300 ng/mL Female:10-150 ng/mL • Serum Iron: Male (80-180 mcg/dL) Female (60-160mcg/dL). • Total Iron-Binding Capacity (TIBC): 250-460 mcg/dL. • Transferrin: Male (215-365 mg/dL) Female (250-380 mg/dL) • Transferrin Saturation: Male 20% to 50% Females 15% to 50% • Hematocrit: Male 42%-52% Female 37%-47% • Hemoglobin: Male14-18g/dL Female12-16g/dL
Laboratory Tests: Ferritin • Most sensitive test to determine iron-deficiency anemia • Major iron-storage protein, normally present in the serum in concentrations directly related to iron storage • Decreases in ferritin levels indicate a decrease in iron storage associated with iron deficiency anemia • Ferritin level below 10mg/100mL is diagnostic of iron deficiency anemia • Only when protein depletion is severe can ferritin be decreased by malnutrition • Ferritin can act as acute-phase reactant protein and may be elevated in conditions not reflecting iron stores
Laboratory Tests : Serum Iron • Serum iron: measurement of the quantity of iron bound to transferrin (globulin protein transporting absorbed iron from the plasma to the bone marrow to be incorporated into Hgb). • Decreased serum iron level is characteristic of iron-deficiency anemia. • Serum iron levels may vary significantly during the day • Blood specimen should be drawn in the morning • Refrain from eating for appx. 12 hrs to avoid high iron measurement by eating food with a high iron content
Laboratory Test: TIBC and Transferrin • TIBC is a measurement of all proteins available for binding mobile iron. • Transferrin represents the largest quantity of iron-binding proteins. • Thus TIBC is an indirect yet accurate measurement of transferrin. • Ferritin not included in TIBC (binds only stored iron) • TIBC is increased in 70% of patients with iron deficiency. • During iron overload, TIBC is less reflective of true transferrin levels
Laboratory Test: TIBC and Transferrin Saturation • Transferrin saturation (%)= Serum iron level x (100%)TIBC • Percentage of transferrin and other mobile iron-binding proteins saturated with iron is helpful in determining the cause of abnormal iron and TIBC levels. • Decreased TIBC saturation or transferrin saturation level is characteristic of iron-deficiency anemia (decreased below 15%) • Increased intake or absorption of iron leads to elevated iron levels (TIBC is unchanged and the percent of transferrin saturation increases)
Laboratory Tests: Iron-related CBC • Hematocrit (Hct)-measure of the percentage of total blood volume that is made up by the RBCs. • Decreased levels of Hct indicate anemia. • Hctcan be altered by dehydration, increased RBC size, pregnancy due to chronic hemodilution, living at high altitudes. • Hemoglobin (Hgb)-measure of the total amount of Hgb in the blood. Oxygen carrying capacity of the blood determined by the Hgb concentration • Decreased levels of Hgb indicate anemia • Hgblevels can be altered during pregnancy, living in high altitudes, being a heavy smokes. • Red Blood Cell Count (RBC)- count of the number of circulating RBCs in 1 mm3 of peripheral venous blood. • When the value is decreased by more than 10% of the expected normal value, the patient is said to be anemic. • RBC alters with pregnancy, high altitudes, and hydration status.
Laboratory Tests: Hemoglobin • Hgb concentration by itself unsuitable as a diagnostic tool in cases of suspected iron deficiency anemia • It is affected only late in the disease • It cannot distinguish iron deficiency from other anemias • Hemoglobin values in normal individuals vary widely
Laboratory Tests: protoporphyrin • The iron-containing portion of the respiratory pigments that combine with protein to form hemoglobin or myoglobin can be used to assess iron deficiency • The zinc protoporphryin (ZnPP)/heme ratio is measured • This can be affected by chronic infection • Can produce a condition that mimics iron deficiency anemia when iron is adequate
Pathophysiology • Depleted iron stores, inadequate iron delivery to bone marrow, impaired iron use within the marrow causes reduced hgb synthesis • Iron deficiency anemia present when the demand for iron exceeds the supply • Develops slowly through four overlapping stages • Stage I: Early negative iron balance • Stage II: Iron stores are depleted. Erythropoiesis proceeds normally with the hgb content of RBCs remaining normal • Stage III: Decreased circulating iron levels; thus transportation of iron to bone marrow is diminished resulting in damaged metabolism and iron deficiency erythropoiesis (decreased levels of erythron iron) • Stage IV: more small hemoglobin-deficient cells enter the circulation in sufficient numbers to replace the normal mature erythrocytes that have been removed from the circulation
Signs and Symptoms • More severe epithelial disorders: • Red, sore, painful tongue • Brittle, thin, spoon shaped (koilonychia) nails • Mouth: atrophy of lingual papillae- glossitis; burning; redness; angular stomatitis; and a form of dysphagia • Stomach: gastritis, may result in achloryhdria • Skin may appear pale • Inside of lower eyelid may be light pink instead of red • Cardiovascular and respiratory changes can lead to cardiac failure • Fatigue, shortness of breath • Decreased work performance/exercise tolerance • Anorexia • Pica • Pagophagia (ice eating) • Slow cognitive and social development in children • Growth abnormalities • Reduction in gastric acidity • Reduced immunocompetence • Mental confusion, memory loss, disorientation in elderly population
Screening Strategies • Physical signs may not appear until stage III or IV • Important to screen those individuals who are at risk • Measurement of serum ferritin levels may best reveal stages I and II negative iron balance • Serum TIBC may also be as good an indicator
Risk for Iron Deficiency Anemia • Infants • Adolescent girls • Childbearing years/pregnancy for women • Older Adults • Those living in chronic poverty • Female athletes (esp. involve in endurance sports)
Treatment of Iron Deficiency Anemia • Treatment should focus on underlying disease leading to the anemia. Repletion of the iron stores, not merely alleviation of the anemia • Chief treatment: oral administration of inorganic iron in the ferrous form • Most widely used preparation is ferrous sulfate • Other salts absorbed to about the same degree are ferrous forms of lactate, fumarate, glycine sulfate, glutamate, and gluconate • Iron best absorbed when stomach is empty (although this can cause gastric irritation) • GI side effects: nausea, heartburn, diarrhea, constipation, epigastric discomfort and distention • If this happens, patients should take iron with meals, though this will reduce absorbability
Continued • Health professional generally prescribe oral iron for iron deficiency for 3 months (taken 3 times daily) • Depending on the severity of the anemia and tolerance of iron supplementation, a daily dose should be 50 to 200 mg for adults and 6 mg/kg for children • Ascorbic acid increases both iron absorption and iron gastric irritation • Absorption of 10 to 20 mg of iron per day permits RBC production to increase to about 3x the normal rate and increase hgb concentration .2g/dL • Increased reticulocytosis is seen within 2 to 3 days, hgb level will begin to increase by day 4 of treatment • Iron supplementation should be continued for 4 to 5 months to allow for repletion of body iron reserves
Continued • If iron supplements don’t correct the anemia: • 1. patient may not be taking the medication as prescribed, most likely because of side effects • 2. bleeding may be be continuing at a rate faster than erythroid marrow can replace the blood cells • 3. the supplemental iron may not be absorbed 2° to steatorrhea, celiac disease, or hemodialysis. • In these circumstances parenteral administration of iron in the form of iron-dextran may be necessary
Bioavailability of Iron • Rate of absorption depends on iron status of individual • The lower the iron stores, the greater the rate of absorption will be. • Iron absorption averages about 5 to 15% from diet of both heme and nonheme iron in a person with normal iron stores • Absorption in iron deficiency often increases iron absorption to about 20 to 30% • Absorption can be as high as 50% in iron deficiency anemia although not common
Bioavailability of Iron • Efficiency of iron absorption determined somewhat by food that it is derived from • Heme iron is much better absorbed than nonheme iron • About 3 to 8% of nonheme iron is absorbed • About 15% of heme iron is absorbed • The ferrous form of nonheme iron is better absorbed than ferric iron • Not all ferrous compounds are equally available. Ferrous pyrophosphate used in breakfast cereals is used often because it doesn’t add a gray color to food but it is poorly absorbed • Ascorbic acid improves iron absorption (reduces ferric to ferrous iron and forms a chelate with iron remaining soluble throughout lower SI)
Bioavailability of Iron • Animal proteins enhance absorption by an unknown mechanism • Gastric acidity enhances solubility and bioavailability of iron from foods; administration of alkaline substances can interfere with nonheme absorption • High phytate, oxalates, and tannin content in foods inhibit absorption of nonheme iron (avoid tea and coffee with meals) • Increased intestinal motility decreases contact time and removes chyme from highest intestinal acidity, decreasing absorption • Poor fat digestion leading to steatorrhea also decreases iron absorption
Food Sources of Iron • Best source of dietary iron is liver. • Followed by seafood, kidney, heart, lean meat, and poultry • Dried beans and vegetables are the best plant sources • Other foods: egg yolks, dried fruits, dark molasses, whole grain and enriched breads, wine and cereal • Milk devoid of iron • Corn poor source of iron • Iron skillet used for cooking add to total iron intake
Intake of Iron • RDA: • Men and postmenopausal women: 8 mg/day • Women of childbearing age: 18 mg/day • Teenage boys: 11 mg/day • Median iron intakes of most women are lower than the RDA, and the median intakes of men generally exceed the RDA. • Foods that supply the greatest amount of iron in US diet include ready to eat cereals fortified with iron; bread, cakes, cookies, doughnuts, and pasta (all fortified with iron); beef; dried beans and lentils; and poultry. • Iron fortification of cereals, flours, and bread has added significantly to the total iron intake of the US. • Concern about potential iron overloading from fortified breakfast foods was raised because analyzed values of iron content were greater than labeled values
Iron Overload • Concern with excessive iron intake is related to its role in coronary heart disease and cancer • Excessive iron can contribute to an enriched oxidative environment that favors • oxidation of LDL cholesterol • arterial vessel damage • other adverse effect affecting the cardiovascular system
Iron Overload • Major cause of iron overload is hereditary hemochromatosis • Overload is linked to a distinct gene that favors excessive iron absorption when iron is available in the diet • Frequent blood transfusions or long term ingestion of large amounts of iron can lead to abnormal accumulation of iron in the liver • Saturation of tissue apoferritin with iron is followed by the appearance of hemosiderin (storage form for iron but contains more iron than ferritin and is very insoluble) • Hemosiderosis (iron storage condition) associated with tissue damage is considered hemochromatosis • This tissue damage can result in progressive hepatic, pancreatic, cardiac, and other organ damage • Absorb 3x more iron from their food than normal
Iron overload Treatment/MNT • Treatment for significant iron overload: • Weekly phlebotomy for 2 to 3 years may be required to eliminate all excess iron • May also involve iron depletion with intravenous desferrioxamine-B • Calcium disodium ethylenediaminetetraactic acid can also be used • MNT: • Ingest less heme iron compared with nonheme iron • Avoid alcohol and vitamin C supplements because both enhance iron absorption • Avoid foods highly fortified with iron, iron supplements, or multiple vitamins/mineral supplements that contain iron • RDA should not be exceeded
Pathophysiology • B12is freed from protein (by way of gastric secretions) • B12binds to R-protein • R-protein hydrolyzed in sm. Intestine • Intrinsic factor bind to B12 • IF binds to specific membrane receptor on illeulbrush border • B12is absorbed • B12binds to transcobalamins (TCI, TCII, etc)
Etiology Not enough B12 in diet • strict vegan • chronic alcoholism • poverty • religion Inadequate use • B12 antagonist • enzyme deficiency • abnormal binding proteins • inadequate binding proteins Increased Requirement • hyperthyroidism • hematopoiesis • infancy Increase excretion • liver disease • renal disease • inadequate binding protein Poor Absorption • Gastric disorders • Addisonian Pernicious Anemia • hereditary, defective, autoimmunity • gastrectomy • total • subtotal • antibody to IF • blocking • binding • sm. intestine disorders • celiac • tropical sprue • strictures, lesions, resection • specific malabsorptions • competition for B12 • bacteria(H. pylori) • pancreatic disease • HIV
S/S Gastrointestinal Tract • Decr. gastric secretions • decr. breakdown of protein-->lower amt of B12 • incr. bac count Other • fatigue • diarrhea • shortness of breath • nervousness Central/peripheral nervous system • paresthesia(demylination) • reduction of senses • decr. muscle coordination • decr. memory • incr. risk for osteoporosis
Diagnosis • Radio assays measure B12and folatetogether • IF antibody • dUsuppression test • serum homocysteine & serum methionine • anti-parietal cell antibodies • low holoTCII (early sign)