Download
1 / 1
10 likes | 77 Vues
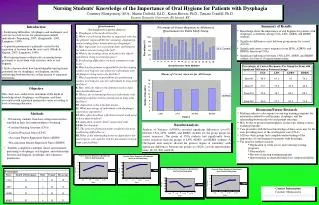
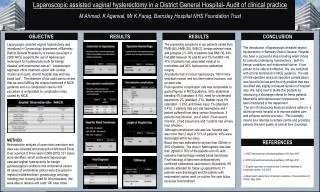
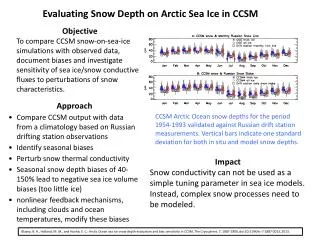
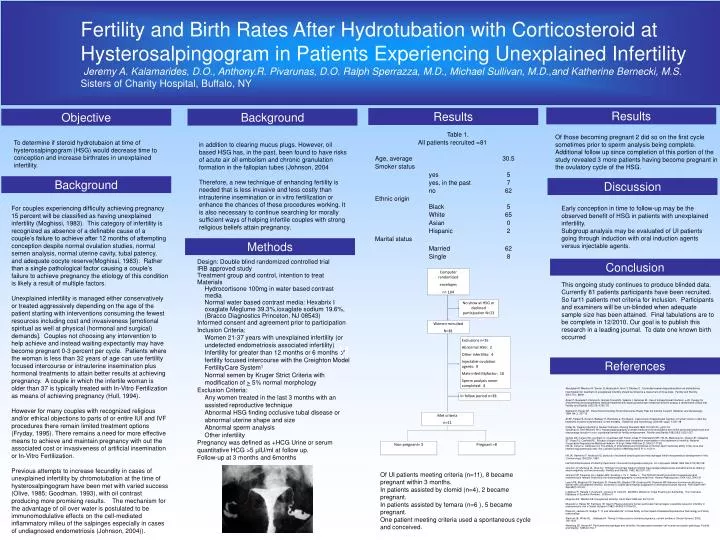
Computer randomized envelopes n= 104. No show at HSG or declined participation N=23. Women recruited N=81. Exclusions n=35 Abnormal HSG: 2 Other infertility: 4 Injectable ovulation agents: 9 Male infertilityfactor: 16 Sperm analysis never completed: 4. In follow period n=38.

E N D
Computer randomized envelopes n= 104 No show at HSG or declined participation N=23 Women recruited N=81 Exclusions n=35 Abnormal HSG: 2 Other infertility: 4 Injectable ovulation agents: 9 Male infertilityfactor: 16 Sperm analysis never completed: 4 In follow period n=38 Met criteria n=11 Non-pregnant= 3 Pregnant =8 Fertility and Birth Rates After Hydrotubation with Corticosteroid at Hysterosalpingogram in Patients Experiencing Unexplained Infertility Jeremy A. Kalamarides, D.O., Anthony.R. Pivarunas, D.O. Ralph Sperrazza, M.D., Michael Sullivan, M.D.,and Katherine Bernecki, M.S. Sisters of Charity Hospital, Buffalo, NY Results Results Objective Background Of those becoming pregnant 2 did so on the first cycle sometimes prior to sperm analysis being complete. Additional follow up since completion of this portion of the study revealed 3 more patients having become pregnant in the ovulatory cycle of the HSG. To determine if steroid hydrotubaion at time of hysterosalpingogram (HSG) would decrease time to conception and increase birthrates in unexplained infertility. in addition to clearing mucus plugs. However, oil based HSG has, in the past, been found to have risks of acute air oil embolism and chronic granulation formation in the fallopian tubes (Johnson, 2004 Therefore, a new technique of enhancing fertility is needed that is less invasive and less costly than intrauterine insemination or in vitro fertilization or enhance the chances of these procedures working. It is also necessary to continue searching for morally sufficient ways of helping infertile couples with strong religious beliefs attain pregnancy. Background Discussion For couples experiencing difficulty achieving pregnancy 15 percent will be classified as having unexplained infertility (Moghissi, 1983). This category of infertility is recognized as absence of a definable cause of a couple’s failure to achieve after 12 months of attempting conception despite normal ovulation studies, normal semen analysis, normal uterine cavity, tubal patency, and adequate oocyte reserve(Moghissi, 1983). Rather than a single pathological factor causing a couple’s failure to achieve pregnancy the etiology of this condition is likely a result of multiple factors. Unexplained infertility is managed either conservatively or treated aggressively depending on the age of the patient starting with interventions consuming the fewest resources including cost and invasiveness [emotional spiritual as well at physical (hormonal and surgical) demands]. Couples not choosing any intervention to help achieve and instead waiting expectantly may have become pregnant 0-3 percent per cycle. Patients where the woman is less than 32 years of age can use fertility focused intercourse or intrauterine insemination plus hormonal treatments to attain better results at achieving pregnancy. A couple in which the infertile woman is older than 37 is typically treated with In-Vitro Fertilization as means of achieving pregnancy (Hull, 1994). However for many couples with recognized religious and/or ethical objections to parts of or entire IUI and IVF procedures there remain limited treatment options (Fryday, 1995). There remains a need for more effective means to achieve and maintain pregnancy with out the associated cost or invasiveness of artificial insemination or In-Vitro Fertilization. Previous attempts to increase fecundity in cases of unexplained infertility by chromotubation at the time of hysterosalpingogram have been met with varied success (Olive, 1985; Goodman, 1993), with oil contrast producing more promising results. The mechanism for the advantage of oil over water is postulated to be immunomodulative effects on the cell-mediated inflammatory milieu of the salpinges especially in cases of undiagnosed endometriosis (Johnson, 2004)). Early conception in time to follow-up may be the observed benefit of HSG in patients with unexplained infertility. Subgroup analysis may be evaluated of UI patients going through induction with oral induction agents versus injectable agents. Methods • Design: Double blind randomized controlled trial • IRB approved study • Treatment group and control, intention to treat • Materials • Hydrocortisone 100mg in water based contrast media • Normal water based contrast media: Hexabrix I oxaglate Meglume 39.3%,ioxaglate sodium 19.6%, (Bracco Diagnostics Princeton, NJ 08543) • Informed consent and agreement prior to participation • Inclusion Criteria: • Women 21-37 years with unexplained infertility (or undetected endometriosis associated infertility) • Infertility for greater than 12 months or 6 months of fertility focused intercourse with the Creighton Model FertilityCare System1 • Normal semen by Kruger Strict Criteria with modification of > 5% normal morphology • Exclusion Criteria: • Any women treated in the last 3 months with an assisted reproductive technique • Abnormal HSG finding occlusive tubal disease or abnormal uterine shape and size • Abnormal sperm analysis • Other infertility • Pregnancy was defined as +HCG Urine or serum quantitative HCG >5 µIU/ml at follow up. • Follow-up at 3 months and 6months Conclusion This ongoing study continues to produce blinded data. Currently 81 patients participants have been recruited. So far11 patients met criteria for inclusion. Participants and examiners will be un-blinded when adequate sample size has been attained. Final tabulations are to be complete in 12/2010. Our goal is to publish this research in a leading journal. To date one known birth occurred M References Aboulghar M, Mansour R, Serour G, Abdrazek A, Amin Y, Rhodes C. Controlled ovarian Hyperstimulation an dintrauterine insemination for treatmetn of unexplained infertility should be limited to a maxiumum of three trials. Fertility and Sterility. 2001:75;1, 88-91 Acien P, Quereda F, Campos A, Gomez-Torres MJ, Velasco I, Gutierrez M. Use of intraperitoneal interferon -2b therapy for endometriosi and postoperative medical treatment with depot gonadotropin releasing hormone analog: a randomized clinical trial. Fertility and Sterility 2002:78; 4:705-711 Agarwal S, Haney AF. Does Recommending Timed Intercourse Really Help the Infertile Couple? Obsterics and Gynecology. 1994: 84; 2, 307-10 Ali AF, Fateen B, Ezzet A, Badawy H, Ramadan a, El-tobge A. Laproscopic intraperitoneal injection of human inferon -2bin the treatment of pelvic endometriosis: a new modality. Obstetrics and Gynecology. 2000:95; suppl. 1;S47-48 Friday M, Treating Infertility in Roman Catholics, Nursing Standard 1995:10;5 (25-31), pp31-34 Goodman S, Rein Mitchell, Hill j. Hysterosalpingography contrast media and chromotubation dye inhibit peritoneal lymphocyte and macrophage function in vitro: a potential benefit for fertility enhancement. Fertility and Sterility 1993:59;5,1022-1027 Guzick DS; Carson SA; Coutifaris C; Overstreet JW; Factor-Litvak P; Steinkampf MP; Hill JA; Mastroianni L; Buster JE; Nakajima ST; Vogel DL; Canfield RE. Efficacy of superovulation and intrauterine insemination in the treatment of infertility. National Cooperative Reproductive Medicine Network. N Engl J Med 1999 Jan 21;340(3):177-83 Hill JA, Cohen J, Anderson DJ. The effects of lymphokines and monokines on human sperm fertilizing ability in the zona-free hamster egg penetration test. Am J obstet Gynecol 1989 May;160(5 Pt 1):1154-9 Hill JA, Haimovici F, Anderson Dj: products of activated lymphocytes and macrophages inhibit mouseembryo development in-vitro. J immunology.139:2250, 1987 Hull MG Effectiveness of infertility treatments: choice and comparative analysis. Int J Gynaecol Obstet 1994 Nov;47(2):99-108 Johnson JV, Montoya IA, Olive DL. Ethiodol oil contrast medium inhibits macrophage phagocytosis and adherence by altering electronegativity and microviscosity. Fertility and Sterility. 1992, 58;3:511-517 Johnson NP, Farquhar cm, Hadden WE, Suckling J, Yu Y, Sadler L. The FLUSH trial with Lipiodolfor Unexplained (and endometriosis-related) Subfertility by Hysterosalpingography: a randomized trial. Human Reproduction. 2004:19;9, 2043-51 Leach RE; Moghissi KS; Randolph JF; Reame NE; Blacker CM; Ginsburg KA; Diamond MP Intensive hormone monitoring in women with unexplained infertility: evidence for subtle abnormalities suggestive of diminished ovarian reserve. Fertil Steril 1997 Sep;68(3):413-20. Luttjeboer F, Harada T, Hughes E, Johnson N, Lilford R, Mol BWJ, Watson A. Tubal Flushing for Subfertility. The Cochrane Database of Systemic Reviews. 2008:vol 1 Moghissi KS; Wallach EE Unexplained infertility. Fertil Steril 1983 Jan;39(1):5-21 Muscato IJ, Haney AF, Eeinberg IB. Sperm Phagocytostis by human peritoneal macrophages: a possible cause for infertility in endometriosis. Am J Obstet Gynencol 1982;144:503-10Olive DL, Peters K, Jackson D, Rudge T. “It Just Alienated Us”: A Case Study on the impact of Assisted Reproductive Technology on Family relationships Stanford JB, White GL, , Hatasaka H. Timing of intercourse to achieve pregnancy: current evidence. Obstet Gynecol. 2002; 100:1333 Weinberg JB, Haney AF. Peritoneal macrophages and infertility: the association between cell number and pelvic pathology. Fertility and Sterility. 1985;44:772-7 Of UI patients meeting criteria (n=11), 8 became pregnant within 3 months. In patients assisted by clomid (n=4), 2 became pregnant. In patients assisted by femara (n=6 ), 5 became pregnant. One patient meeting criteria used a spontaneous cycle and conceived.