Download
1 / 1
10 likes | 220 Vues
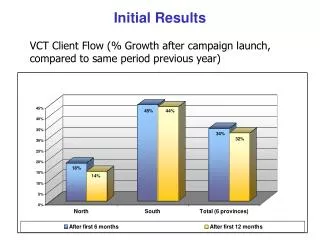
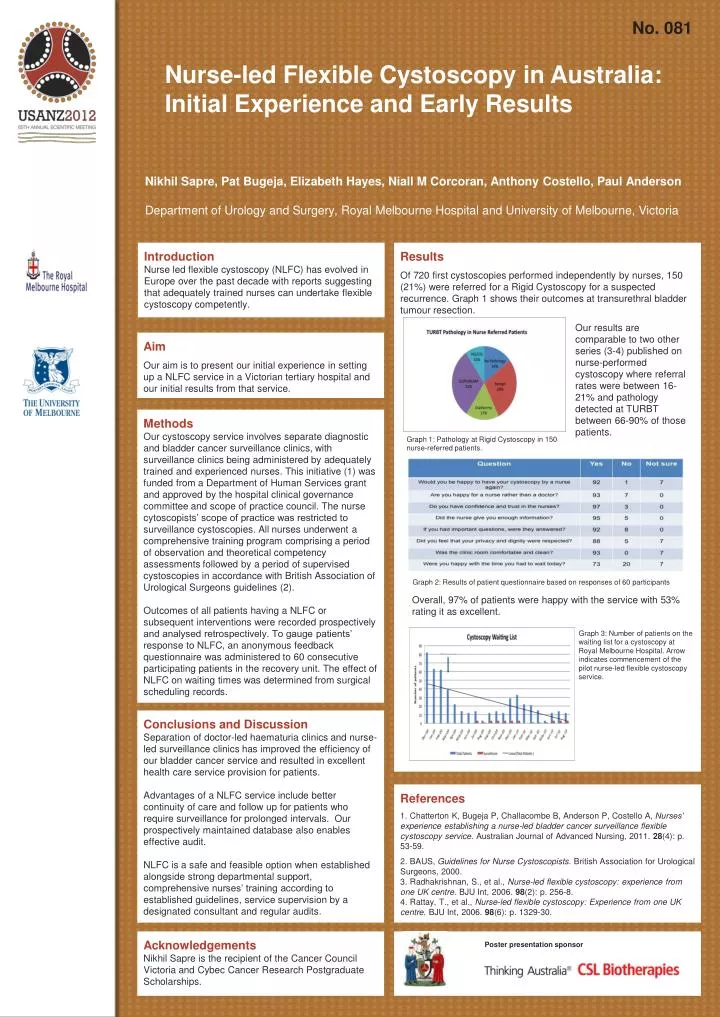
No. 081. Nurse-led Flexible Cystoscopy in Australia: Initial Experience and Early Results. Nikhil Sapre , Pat Bugeja , Elizabeth Hayes, Niall M Corcoran, Anthony Costello, Paul Anderson Department of Urology and Surgery, Royal Melbourne Hospital and University of Melbourne, Victoria.

E N D
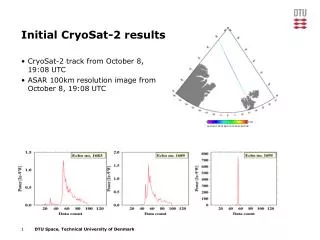
No. 081 Nurse-led Flexible Cystoscopy in Australia: Initial Experience and Early Results Nikhil Sapre, Pat Bugeja, Elizabeth Hayes, Niall M Corcoran, Anthony Costello, Paul Anderson Department of Urology and Surgery, Royal Melbourne Hospital and University of Melbourne, Victoria Introduction Nurse led flexible cystoscopy (NLFC) has evolved in Europe over the past decade with reports suggesting that adequately trained nurses can undertake flexible cystoscopy competently. Results Of 720 first cystoscopies performed independently by nurses, 150 (21%) were referred for a Rigid Cystoscopy for a suspected recurrence. Graph 1 shows their outcomes at transurethral bladder tumour resection. Our results are comparable to two other series (3-4) published on nurse-performed cystoscopy where referral rates were between 16-21% and pathology detected at TURBT between 66-90% of those patients. Aim Our aim is to present our initial experience in setting up a NLFC service in a Victorian tertiary hospital and our initial results from that service. Methods Our cystoscopy service involves separate diagnostic and bladder cancer surveillance clinics, with surveillance clinics being administered by adequately trained and experienced nurses. This initiative (1) was funded from a Department of Human Services grant and approved by the hospital clinical governance committee and scope of practice council. The nurse cytoscopists’ scope of practice was restricted to surveillance cystoscopies. All nurses underwent a comprehensive training program comprising a period of observation and theoretical competency assessments followed by a period of supervised cystoscopies in accordance with British Association of Urological Surgeons guidelines (2). Outcomes of all patients having a NLFC or subsequent interventions were recorded prospectively and analysed retrospectively. To gauge patients’ response to NLFC, an anonymous feedback questionnaire was administered to 60 consecutive participating patients in the recovery unit. The effect of NLFC on waiting times was determined from surgical scheduling records. Graph 1: Pathology at Rigid Cystoscopy in 150 nurse-referred patients. Graph 2: Results of patient questionnaire based on responses of 60 participants Overall, 97% of patients were happy with the service with 53% rating it as excellent. Graph 3: Number of patients on the waiting list for a cystoscopy at Royal Melbourne Hospital. Arrow indicates commencement of the pilot nurse-led flexible cystoscopy service. Conclusions and Discussion Separation of doctor-led haematuria clinics and nurse-led surveillance clinics has improved the efficiency of our bladder cancer service and resulted in excellent health care service provision for patients. Advantages of a NLFC service include better continuity of care and follow up for patients who require surveillance for prolonged intervals. Our prospectively maintained database also enables effective audit. NLFC is a safe and feasible option when established alongside strong departmental support, comprehensive nurses’ training according to established guidelines, service supervision by a designated consultant and regular audits. References 1. Chatterton K, Bugeja P, Challacombe B, Anderson P, Costello A, Nurses’ experience establishing a nurse‐led bladder cancer surveillance flexible cystoscopy service. Australian Journal of Advanced Nursing, 2011. 28(4): p. 53-59. 2. BAUS, Guidelines for Nurse Cystoscopists. British Association for Urological Surgeons, 2000. 3. Radhakrishnan, S., et al., Nurse-led flexible cystoscopy: experience from one UK centre. BJU Int, 2006. 98(2): p. 256-8. 4. Rattay, T., et al., Nurse-led flexible cystoscopy: Experience from one UK centre. BJU Int, 2006. 98(6): p. 1329-30. Acknowledgements Nikhil Sapre is the recipient of the Cancer Council Victoria and Cybec Cancer Research Postgraduate Scholarships. Poster presentation sponsor