Download
1 / 56
680 likes | 862 Vues
Antibodies as Immune Modulators: Combinatorial Immunotherapy of Cancer. Madi R. Madiyalakan , PhD Chief Executive Officer. Quest PharmaTech Inc. 8123 Roper Road NW, Edmonton, Alberta, Canada. Company Overview. Quest PharmaTech is a publicly traded Canadian biotechnology company

E N D
Antibodies as Immune Modulators:Combinatorial Immunotherapy of Cancer Madi R. Madiyalakan, PhD Chief Executive Officer Quest PharmaTech Inc. 8123 Roper Road NW, Edmonton, Alberta, Canada
Company Overview • Quest PharmaTech is • a publicly traded Canadian biotechnology company • developing a portfolio of product candidates for the treatment of cancer • by combining proprietary antibodies with • chemotherapy • immuno-stimulants • photodynamic therapy • Oregovomab for treatment of Ovarian Cancer is in a 80 patients Phase II clinical trial
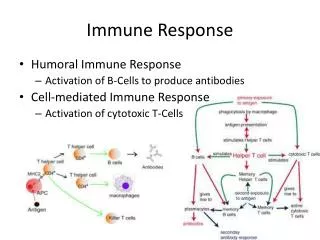
Quest’s Approach For Cancer Treatment Cancer immunotherapy Proprietary use of Anti-cancer Antibodies as Immune Modulators Combinatorial Immunotherapy is superior to Mono-immunotherapy Engineered anti-cancer IgE antibodies may be comparable, complementary, or even superior to their IgG counterparts
Cancer Immunotherapy • Enlisting the body to fight cancer • Stimulating your own immune system to work harder and/or smarter • Increase the specificity and amount of anti-cancer immunologic factors
Renewed Optimism For Immunotherapy of Cancer: Newest Approvals • In 2010 two immunotherapy products were approved for cancer treatment • Provenge (Sipuleucel T) by Dendreon, an autologus dendritic cell therapy for prostate cancer • Yervoy(Ipilimumab) by BMS, a checkpoint blockade inhibiting antibody for melanoma • Unifying lesson • Tumor directed immunity can treat cancer • Tumor specific T cells in a favorable immune regulatory state can control advanced cancer
Antibodies as Immunemodulators Most Therapeutic Antibodies used as “drugs” Developed based on Receptor Targeting and interference Pharmacological Dose response requiring high administered doses based on molecular weight (examples Herceptin, Avastin, Rituxan, etc) In contrast, Quest uses IgG to induce immunity to target Self Antigens (lower immunologic dose)
Antibodies as Immunemodulators Low dose (about 2 mg), intravenous administration of a xenotypic antibody to TAA After injection, antibody binds to cancer antigen and forms immune complexes The complexes are cross processed and presented by dendritic cells to activate T-cells CA125-B43.13 Complex CA125 conjugated with FITC (green) pre-incubated with MAb-B43.13-Cy3 (red) added to day 5 DC for 30 min. before fixation; yellow: co-localized complex
Antibodies as ImmunemodulatorsAnti-MUC1 Ab Clinical Experience MUC1 is a dominant tumor antigen on most adenocarcinoma Colon, lung, pancreas, ovary, pancreas, multiple myeloma, others Mucinous glycoprotein differentially expressed in malignant tissue hypoglycosylated in malignancy and expressed on all cell surfaces a distinct immune target
MAb AR20.5 Clinical Studies: Phase I Objectives: • To determine the safety of MAb AR20.5 administered intravenously on weeks 1, 3, 5, 9, 13, and 17 at 3 defined dose levels • To assess the humoral and cellular immune responses induced by MAb AR20.5 • To assess preliminary anti-tumor responses
MAb AR20.5 Clinical Studies: Phase IImmunological Response Results Summary: HAMA, Ab2, anti-MUC1 antibodies and T-cells were induced in 26-40 % of patients across all dose levels Two patients at the 2 mg dose level experienced a decrease in the CA 15.3 level of 29.5 % and 37.6 % A correlation was found between development of anti-MUC1 antibodies and T-cells with stabilization or decrease of CA15.3 de Bono et al Annals of Oncology 2004; 15:1825-1833
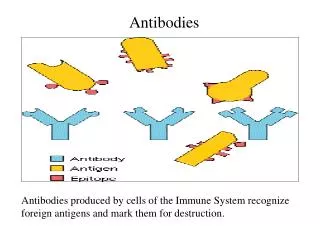
Antibodies as Immune Modulators:Conclusion Injection of antibodies against tumor association antigens can induce antigen specific T cell response (through cross presentation) which also correlates with clinical response
Ovarian Cancer & CA125 The Therapeutic Demand Common and Fatal: this is the fifth most common cause of cancer death in women in the US with the highest mortality rate of gynecological tumors Late Diagnosis: approximately 70% of patients present with advanced disease (Stage III/IV) at the time of diagnosis Poor Prognosis: the 5 year survival rate is 20% for stage III, and only 5% for stage IV No Cure: treatment includes surgery, chemotherapy Need for an effective low toxicity therapy that leads to a longer better life CA125 is large glycosylated protein, also known as MUC16 Expressed on cell surface of serous epithelial ovarian cancer cells Shed into the circulation Used in diagnosis and to monitor progress of disease and treatment
Lead Product: Oregovomab (MAb-B43.13) for CA125 Associated Cancer Antigen specificity CA125 Isotype Mouse IgG1κ Affinity 1.1x1010 M-1 for CA125 antigen Immunohistochemistry Stains specifically ovarian and pancreatic carcinomas expressing CA125 No direct effects (ADCC, CDC, receptor blockage)
Oregovomab Initial Clinical Studies (Done by Unither Pharmaceuticals)
Oregovomab Clinical Studies Findings Mono-Immunotherapy is not ideal for Ovarian Cancer Treatment Need for serum Antigen for Antibody Antigen Complex Formation (Cross Presentation) Correlations between Antigen Specific T Cells (ELISPOT) and Survival Chemotherapy Enhances Immune Response
Combinatorial Immunotherapy:The New Frontier Immunotherapy induces minimal toxicity Can act independent of concomitant therapies Can be used in combination with conventional therapies such as chemotherapy, local radiation of tumor, small molecule targeted therapy, photodynamic therapy, etc. Can be used in combination with other immune modulating therapies such as immunoadjuvants, check point inhibitors, T cell adaptive transfer therapy, Danger Signals, etc.
Chemotherapy Enhances Immune Response Positive Immune Interaction In Vitro with Taxol for Induction of CTL Activity Compared to Drug Alone and Necrotic Cells
MAb AR20.5 Therapeutic Animal Model MUC1-Transgenic Mouse Developed by Dr. Gendler, Mayo Clinic, Scottsdale, AZ C57BL/6 mice that express human MUC1 in tissue-specific fashion MUC1-transgenic mice without tumor to optimize the immunization protocol MUC1-transgenic mice with orthotopic and subcutaneous transplantable tumors (Panc02.MUC1) and spontaneously developing tumors for tumor control studies
MAb AR20.5Chemo-enhanced Immunotherapy Potential with Gemcitabine Human MUC1 Transgenic Mice with Subcutaneous Panc02.MUC1 Tumor Model
Chemo-enhanced Immunotherapy:Drug Specific Enhancement Baxeuanis et al Cancer Immunol immunother (2009) 8:317-24
New Perspective:Cytotoxics are Immune Modulators Cytotoxics induce apoptosis and favorable antigen presentation of tumor Cytotoxics can reduce Regulatory T cell Burden Cytotoxics can influence the character of an induced response in an agent specific manner.
Chemo-enhanced immunotherapy in Advanced Ovarian Cancer Patients:A Phase II Clinical Study
Oregovomab Chemo Enhanced Immunotherapy Front-line Chemo-enhanced Immunotherapy Pilot Phase II Study Design Arm A: concurrent with chemotherapy (Treatment) Arm B: one week following chemotherapy (Control) Braly et al J Immunother 2009;32:54–65
Oregovomab Chemo Enhanced Immunotherapy Front-Line Chemo-enhanced Immunotherapy Pilot Phase II Study: Kinetics of Immune Response with Chemo-immunotherapy, Influence of Dose Schedule and Comparison to Previous Maintenance Study Arm A: concurrent with chemotherapy (Treatment) Arm B: one week following chemotherapy (Control) Braly et al J Immunother 2009;32:54–65
Oregovomab Chemo Enhanced Immunotherapy Front-Line Chemo-enhanced Immunotherapy Pilot Phase II Study: Kaplan-Meier Curves of Progression-Free Survival by Treatment Arm (ITT) Arm A: concurrent with chemotherapy (Treatment) Arm B: one week following chemotherapy (Control) Braly et al J Immunother 2009;32:54–65
Oregovomab Chemo Enhanced Immunotherapy Front-line Chemo-enhanced Immunotherapy Pilot Phase II Study: CA125-specific T cell Immune Response Arm B: one week following chemotherapy (Control) Arm A: concurrent with chemotherapy (Treatment) 44% 21% Braly et al J Immunother 2009;32:54–65
Oregovomab Chemo Enhanced Immunotherapy Front-line Chemo-enhanced Immunotherapy Pilot Phase II Study: Favorable Clinical Outcome Correlates to Generation of CA125-specific T-cell Response Responders n=11, Non-responders n=24 Braly et al J Immunother 2009;32:54–65
Oregovomab Chemo Enhanced Immunotherapy Study OVA-Gy-12: CA125 Tumor Specific T Cell Induction Associated with Survival Advantage Recurrent /Refractory Disease Population Responders n=11, Non-responders n=7 Gordon et al, 2004
Oregovomab Chemo Enhanced ImmunotherapyConclusion Chemotherapy can be immune enhancing, in a schedule dependent fashion Correlation between T cell response and survival Substantial clinical development supported by phase III product manufacturing development Excellent safety profile Positive clinical data to continue the front-line chemo-immunotherapy study
Oregovomab Chemo Enhanced ImmunotherapyOngoing Clinical Study • Objective: • Confirm clinical signals suggested in Pilot Phase II Oregovomab study to justify a definitive phase III study • Design: • Randomized parallel prospective study of standard chemotherapy vs. standard of care chemotherapy plus oregovomab • Patients: • Newly Diagnosed Stage III/IV CA125 associated Epithelial Ovarian Cancer who have been optimally cytoreduced (n=80)
Oregovomab Chemo Enhanced ImmunotherapyOngoing Clinical Study • Treatment: • Standard of Care Carboplatin Paclitaxel chemotherapy x 6 cycles vs. Standard of Care Carboplatin Paclitaxel chemotherapy x 6 cycles with oregovomab 2mg IV infused at cycle 1, 3, 5 and then at cycle 5 plus 12 weeks • Endpoints: • Safety Profile • CA125 specific ELISPOT • Antibody response (HAMA) • DTH to oregovomab • Progression free survival • Survival
Oregovomab Chemo Enhanced ImmunotherapyOngoing Clinical Study Principle Investigator: Prof Roberto Angioli (University Campus Bio-Medico of Rome) CRO: Dimensione Ricerca, Rome Advisors: Prof Sergio Pecorelli (AIFA) Prof Jonathan Berek (Stanford) Clinical Advisory Board: Dr. Christopher Nicodemus (AIT, US) Professor William McGuire (Inova Fairfax Hospital, US) Professor Ignace Vergote (Catholic University of Leuven, Belgium) Professor Thomas Ehlen (UBC, Canada)
Oregovomab Chemo Enhanced ImmunotherapyOngoing Clinical Study – Clinical Centers
Oregovomab Positioning and Differentiation Potential Competition Targeted Antibodies: Avastin, Farletuzumab Targeted Inhibitors: mTor, PARP Inhibitors Oregovomab is capable of stimulating the patient’s own immune system giving a long lasting effect Novel mechanism of action that targets CA125 tumor marker to elicit T-cells that attack the cancer Should benefit from recent advances in immunotherapy area Benign well tolerated safety profile Good quality of life for patients undergoing therapy
Oregovomab Positioning and Differentiation Relatively simple dose schedule and administration Twenty minute low-dose (2mg) IV infusion 4 – 5 times per year Orphan Drug Designation in US and Europe Fast Track Designation in US; will seek accelerated approval based on PFS and/or tumor specific T cell stimulation Pricing flexibility as Cost of Goods per vial is approximately $150 Target front-line combination chemo-immunotherapy followed by recurrent disease in combination with chemotherapy Expand the market to other CA125 expressing tumors such as pancreatic cancer
Oregovomab Manufacturing Summary(Cell Culture Process Validated at 500 L Scale)
Oregovomab Manufacturing Summary(Downstream Process Validated at 500 L Scale)
Second Generation of Antibody for Immunotherapy Monoclonal IgE to Cancer Antigens
IgE: Another Class of Antibody Plays an important role in allergy Associated with adaptive defense to parasitic organisms Least abundant circulating blood levels among Igs; shares the common light chain of (λ or Κ) Elicits an immune response by binding to Fc receptors High binding affinity for its Fc receptors compared to IgG No monoclonal IgE on the market Monoclonal IgE Next generation antibody therapeutics
Monoclonal IgE For Immunotherapy Inverse correlation between IgE level/allergic history and selected malignancies Chronic anti-IgE therapy associated with increased risk of malignancy Polyclonal IgE levels correlated with survival in multiple myeloma patients IgE positive cellular infiltrate in H&N cancer Specific serum IgE cytotoxic in Pancreatic CA Daniels et al, “The IgE antibody and its use in cancer immunotherapy” in “Cancer and IgE: Introducing the Concept of AllergoOncology” by Penichet, Manuel L.; Jensen-Jarolim, Erika (Eds.) Springer 2010
Proposed Pathways for IgE : Anti-Cancer Effect Tumor specific IgE cause type I hypersensitivity at tumor site, causes local vasodilation and leakage bringing cytotoxic mediators directly to tumor…The antibody will enhance the effects of standard cancer treatments IgE-tumor antigen immune complexes result in enhanced T cell immunity to the antigen ADCP (antibody dependent cell mediated phagocytosis) and ADCC (antibody dependent cell mediated cytoxicity) via relevant Fc-epsilon bearing effectors (including Monocytes, Dendritic cells, Mast cells, Basophils, Eosinophils) (invoking pathways of parasite host defense to fight cancer)
Tumor Protection with Therapeutic anti-Her2 IGE MAb demonstrated In initial animal model studies 100 75 Percent Survival 50 25 15 25 35 45 60 110 Days after D2F2/E2 Challenge Daniels et al, Can. Imm . Immunother. Epub Nov 30, 2011
Anti-PSA IgE (A200)Improves SurvivalCT-26-PSA Tumor Cell Challenged (FcɛRI Transgenic Mouse Model) Daniels et al AACR 2013 & BMC Cancer 2013 in press
Anti-MUC1 IgE 3C6 Delayed Tumor Growth 4T1.hMUC1 Tumor Cell Challenged (hFcɛRI Tg+ Mouse Model) Teo et al Cancer Immunology & Immunotherapy 2012
Combinatory Immunotherapy with addition of TLR Stimulation (Danger Signals)
TLR3 and Cancer Toll-like receptor-3 as a target to enhance bioactivity of cancer (Nicodemus et al, Am J ObstetGynecol 2010;202:608.e1-8) • DC Maturation and T cell stimulation • Augmentation of Oregovomab preclinical effects • Local cytokine induction • Specific B and T cell stimulation to PSA in transgenic-PSA mouse vaccination model • Augmentation of NK mediated cytotoxicity with rituximab • Potential to further enhance activity of all Quest immunotherapy products.
Combinatory Immunotherapy with Photosensitizers Combination with Photodynamic Therapy Generation of local free radicals to enhance immune effector pathways