Download
1 / 17
210 likes | 505 Vues
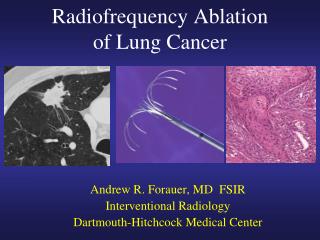
Finite Element Analysis of Radiofrequency Ablation. Abirvab Deb- BME M .E ng ‘14 Brice Lekavich- BME M .E ng ‘14 Cristian Vilorio- BME M .E ng ‘14. Background. Radiofrequency Ablation What is it? Arrhythmias Tumors Varicose Veins.

E N D
Finite Element Analysis of Radiofrequency Ablation Abirvab Deb- BME M.Eng ‘14 Brice Lekavich- BME M.Eng ‘14 Cristian Vilorio- BME M.Eng ‘14
Background Radiofrequency Ablation What is it? Arrhythmias Tumors Varicose Veins "Radiofrequency Ablation (RFA)." Johns Hopkins Medicine. Johns Hopkins Medicine, n.d. Web. 21 Apr. 2014. <http://www.hopkinsmedicine.org/liver_tumor_center/treatments/ablative_techniques/ radio_frequency_ablation.html>.
FEA Motivation • Lesion has to be deep enough into targeted tissue, yet limit the amount of irreversible damage occurring to normal cardiac tissue • The ablated tissue area has to be large enough to compensate for the uncertainties in the electrical mapping that is used to localize the target tissue. • RF energy is effective in ablating some arrhythmias. • Multiple attempts often have to be made prior to successfully destroying the targeted tissue • Lesions produced are not deep enough to eliminate the target electrical pathway • Lesion depth is a problem in the left ventricle where the heart wall is thick
Objective One of the most important reasons to model heat transfer in living tissues is to allow for the prediction of the level and area of potential damage caused by temperature change. • We therefore aim to develop a model that allows for determination of the transient temperature distribution in living tissue under biological conditions and use this distribution to evaluate the potential lesion depth due to radiofrequency ablation. "Control Volume of Tissue Element." Body (Human) Heat Transfer. THERMOPEDIA, 10 Feb. 2011. Web. 20 Apr. 2014. <http://www.thermopedia.com/content/587/>.
FEA Methodology Preprocessing - Geometry generation - Material Properties - Initial Conditions - Boundary Conditions - Mesh Generation Postprocessing - Temperature Distribution - Lesion Dimensions - Convergence Test • Solution • - Duration of RF energy • - Time Steps
Bioheat Transfer & Pennes’ Equation • There are two main approaches to bioheat transfer models: • Continuum approach- thermal impact of all blood vessels is accounted for by perfusion through the effective conductivity of the tissue • Vascular approach- models the impact of each vessel individually, attempting to reproduce the real vascularity of the tissue. • The most widely used continuum model is that given by Harry Pennes (1948). Since then, multiple variations have been developed to improve or account for different factors. • Pennes’ Bioheat Equation:
Assumptions of Pennes’ Equation • Pre-arteriole/post-venule heat transfer between the tissue and blood is neglected. • Blood flow in small capillaries is assumed to be isotropic (ignores blood flow directionality). • Does not consider local vascular geometry (role of larger blood vessels near capillary beds is neglected). • Blood is assumed to reach arterioles supplying the capillary beds at the body core temperature (assumed instantaneous exchange of energy and equilibrium with local tissue temperature). Cardiac cells vascularization Sakaguchi et al. In Vitro Engineering of Vascularized Tissue Surrogates. Scientific Reports 3: 1316, 1-7 (2013).
Modifying Pennes Bioheat Equation • Perfusion Term, Qp • Heat exchanged between the tissue and blood, which is proportional to the product of the volumetric perfusion rate and the difference between the arterial blood entering the tissue and the venous blood leaving the tissue. • Assumption: thermal equilibrium exist between the tissue and venous blood, and arterial blood temperature is equal to core body temperature. • Blood is regarded as a local heat regulator by means of heat convection. • Case 1: Qp is positive = blood acts like a heat source to the tissue • Case 2: Qp is negative = the blood acts as a heat sink to the tissue • *In our case, the core body temperature (Tb) is lower than the tissue temperature (T), and therefore Qp is negative and Case 2 is satisfied.
Modifying Pennes Bioheat Equation • Metabolic Term, Qm • Metabolic heat generation term is considered insignificant compared to the heat generated by the heat source. • Typical values for Qm are around the order of 1000 W/m3, while the heating done by the power source is on the magnitude of 2 to 3 orders higher. • Heat Source, q • There are two different types of ablation— “temperature-controlled” and “voltage-controlled”. For simplification, temperature-controlled ablation was modelled where the electrode tip was held at a constant temperature during ablation.
Governing Equations BCs Temperature: Heat Flux: Convection: Weak form:
Time Integration Have equation of the form: θ-method time integration: Where Plugging and into the θ-family of approximation and rearranging terms to be of the equivalent form of : Where To allow for unconditional stability, (Crank-Nicolson Method) Solve for at each time step.
ANSYS Simulation: Results Contours
ANSYS Simulation: Results Lesion size
Lesion Size after 60sec of Ablation • ~3.5 mm wide • ~2 mm deep • Overall, higher temperature contours hit an equilibrium where heat in is balanced by heat out. • Tissue still continues to heat up as expected at lower temperatures