Download
1 / 24
250 likes | 397 Vues
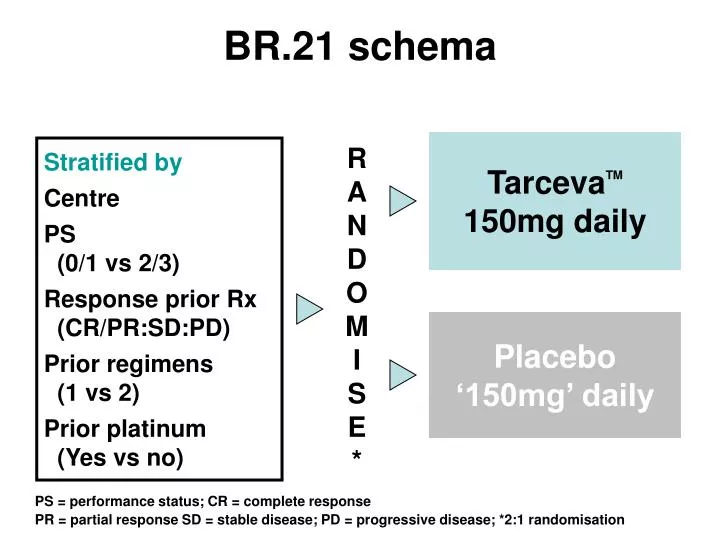
BR.21 schema. Tarceva TM 150mg daily. RANDOM I SE*. Stratified by Centre PS (0/1 vs 2/3) Response prior Rx (CR/PR:SD:PD) Prior regimens (1 vs 2) Prior platinum (Yes vs no). Placebo ‘150mg’ daily. PS = performance status; CR = complete response

E N D
BR.21 schema TarcevaTM150mg daily RANDOM I SE* Stratified by Centre PS (0/1 vs 2/3) Response prior Rx (CR/PR:SD:PD) Prior regimens (1 vs 2) Prior platinum (Yes vs no) Placebo‘150mg’ daily PS = performance status; CR = complete response PR = partial response SD = stable disease; PD = progressive disease; *2:1 randomisation
Study endpoints • Primary • overall survival • Secondary • progression-free survival (PFS) • time to deterioration of cough, dyspnoea, painas per EORTC QLQ-C30 + QLQ-LC13 • response rates, duration • toxicity and tolerability • tissue HER1/EGFR versus outcome and safety • TarcevaTM trough pharmacokinetics HER/EGFR = epidermal growth factor receptor
Key eligibility criteria • Confirmed NSCLC, Stage IIIB or IV • Age ³18 years • PS 0, 1, 2 or 3 • Measurable or non-measurable disease • One or two prior chemotherapy regimens • Adequate organ function • HER1/EGFR+ not required • No prior HER1/EGFR inhibitors • No prior malignancies or uncontrolled CNS M1 • Written informed consent NSCLC = non-small-cell lung cancer; CNS M1 = symptomatic central nervous system metastasis
Overall survival: all patients 1.00 0.75 0.50 0.25 0 42.5% improvement in median survival Survival distribution function HR* = 0.73, p<0.001 HR* = 0.73, p<0.001 TarcevaTM Placebo 0 5 10 15 20 25 30 Survival time (months) *HR and p-value adjusted for stratification factors at randomisation + HER1/EGFR status
Survival after eliminating CR/PRs • Exploratory analyses in BR.21 dataset • The TarcevaTM benefit is still present after eliminating CRs and PRs
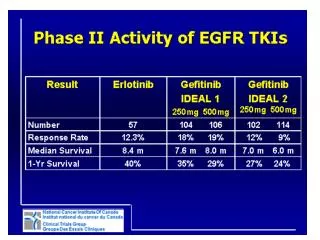
Efficacy data for docetaxel, pemetrexed & erlotinib Ramalingam, S. et al. Oncologist 2006;11:655-665
BR.21: summary of significant clinical predictors of response *Significance between subgroups
BR.21: Survival Across Subgroups Subset n Tarceva: Placebo 731 486 245 PS 0-1 PS 2-3 475 256 Male Female <65 y 65 y 452 279 Adenocarcinoma Squamous cell carcinoma Other histology 365 222 144 Prior weight loss <5% Prior wt loss 5%-10% Prior wt loss >10% 486 132 81 Never smoked Current/ex-smoker 146 545 364 367 1 prior regimen 2 prior regimens 0 0.5 1.0 1.5 2.0 2.5 HR = hash mark on horizontal bar. 95% CI = length of horizontal bar. TARCEVA™ (erlotinib) PI. Decreasedrisk of death Increasedrisk of death
BR.21: Survival Across Subgroups Cont’d Subset n Tarceva: Placebo 731 Prior platinum No prior platinum 678 53 267 464 Prior taxane No prior taxane Best prior response: CR/PR Best prior response: SD Best prior response: PD 292 287 152 <6 mo since diagnosis 6-12 mo since diagnosis >12 mo since diagnosis 97 242 392 EGFR-positive EGFR-negative EGFR unmeasured 127 111 493 Caucasian Asian 567 91 Stage IV at diagnosis Stage <IV at diagnosis 329 402 0 0.5 1.0 1.5 2.0 2.5 HR = hash mark on horizontal bar. 95% CI = length of horizontal bar. TARCEVA™ (erlotinib) PI. Decreasedrisk of death Increasedrisk of death
Clinical Benefit of Erlotinib inMale Smokers with SCCClark, Abstract #7166, Poster NCIC CTG BR.21 : Survival for Male, Ever Smokers with SCC Clark GM et al. ASCO 2006, Abs #7166.
BR.21 Symptom Benefit *Adjustment for multiple testing †Patients were considered to have deteriorated symptoms if the change in score from baseline for each symptom was 10 points or higher at any time-point after baseline assessment
QoL outcomes for second-line therapy 1 Bezjak A, et al. J Clin Oncol 2006;24:3831–7; 2 Dancey J, et al. Lung Cancer 2004;43:183–94; 3 Hanna N, et al. J Clin Oncol 2004;22:1589–97
Comparison of phase III trials in relapsedNSCLC: haematological toxicity Adverse event Tarceva Docetaxel Pemetrexed 2 2 (grade 3/4) (150mg/day) (75mg/m ) (500mg/m ) < Neutropenia 1 40.2 5.3 < Febrile neutropenia 1 12.7 1.9 < Anaemia 1 4.3 4.2 < Thrombocytopenia 1 0.4 1.9 Patients (%) Shepherd F, et al. N Engl J Med 2005;353:123–32 Hanna N, et al. J Clin Oncol 2004;22:1589–97
1st-line Erlotinib in Elderly Patientswith Advanced NSCLCJackman, Abstract #7168 StudyDesign Non-randomized, open label, Phase II trial Jackman DM et al. ASCO 2006, Abs #7168.
1st-line Erlotinib in Elderly Patientswith Advanced NSCLCJackman, Abstract #7168 1.0 0.75 0.50 0.25 0.0 0 26 52 78 104 Survival Median Survival 41 weeks 52-week survival 40.4% Jackman DM et al. ASCO 2006, Abs #7168. Jackman DM et al. 11th WCLC 2005, Abstract #O-188.
1st-line Erlotinib inElderly Patientswith Advanced NSCLCJackman, Abstract #7168 15 15 70 11 24 64 20 22 58 18 9 73 15 15 70 (n=47) (n=45) (n=50) (n=22) (n=37) Symptom Response Poster
1st-line Erlotinib in Elderly Patientswith Advanced NSCLCJackman, Abstract #7168 Results • For the 64 patients eligible for QoL analysis, there was no statistically significant improvement in overall LCSS score. • Patients who achieved PR or SD had statistically significant improvements in their overall score QoL as measured by LCSS. Conclusions • Patients over the age of 70 years had a median survival of 10.9 months when treated with erlotinib in the first-line. • Erlotinib in this population was also associated with improvements in key symptoms of dyspnea, cough, fatigue, pain and loss of appetite. • Improvements in overall LCSS score were noted in patients who achieved disease control (PR or SD). Jackman DM et al. ASCO 2006, Abs #7168.
1st-line Erlotinib in Advanced NSCLCwith Good PrognosisAkerley, Abstract #7178 • Stage IIIb or IV NSCLC • No prior chemotherapy for • metastatic disease • Good prognosis defined as: • No brain metastases • <10% weight loss • O2 use not due to malignancy • PS 0 or 1 • No immediate need for chemotherapy Erlotinib 150 mg/day Objective or symptomatic progression Switch to chemotherapy Study Design Primary Objective Achieve 6-month chemotherapy-progression-free survival rate that is significantly higher than the historically observed 31% Akerley W et al. ASCO 2006, Abs #7178.
1st-line Erlotinib in Advanced NSCLCwith Good PrognosisAkerley, Abstract #7178 Response to Erlotinib n (%) PR 6 (15) SD 11 (28) PD 23 (58) Rash Correlates with Duration of Therapy Grade of Rash Median duration of Tx 0 – 1 7.8 weeks 3 – 4 17.7 weeks Progression-free Survival* 6-month PFS 56% *Chemotherapy-progression-free survival: time from study entry to progression on chemotherapy or erlotinib if patient refused chemotherapy. Subsequent Chemotherapy and Outcomes n (%) Too early to assess 5 (14) Never received chemo 11 (31) PR 9 (26) SD 11 (31) PD 4 (11) Response Akerley W et al. ASCO 2006, Abs #7178.
1st-line Erlotinib in Advanced NSCLCwith Good PrognosisAkerley, Abstract #7178 Overall Survival Akerley W et al. ASCO 2006, Abs #7178.
1st-line Erlotinib in Elderly Patientswith Advanced NSCLCAkerley, Abstract #7178 • Conclusions • The overall response rate was 15%; the 6-month PFS rate is 56%. • Rash predicts the duration of erlotinib effectiveness. • Never smokers show a better survival outcome than ever smokers. • Survival and PFS in this population of minimally selected patients appear comparable to that with chemotherapy. • A randomized trial is warranted to further investigate the results of this trial. Akerley W et al. ASCO 2006, Abs #7178.