Download
1 / 19
230 likes | 507 Vues
Results from the Rheos Pivotal Trial Baroreflex Activation Therapy Sustainably Lowers Blood Pressure in Patients with Resistant Hypertension. John Bisognano , Domenic Sica , Mitra Nadim, Luis Sanchez, George Bakris, On Behalf of the Rheos Pivotal Trial Investigators.

E N D
Results from the Rheos Pivotal Trial Baroreflex Activation Therapy Sustainably Lowers Blood Pressure in Patients with Resistant Hypertension John Bisognano, Domenic Sica, Mitra Nadim, Luis Sanchez, George Bakris, On Behalf of the Rheos Pivotal Trial Investigators
Baroreflex Activation Therapy (BAT) The CVRx Rheos® System Programming System Baroreflex Activation Leads Implantable Pulse Generator
Baroreflex Activation Therapy (BAT) Continuously Modulates the Autonomic Nervous System Carotid Baroreceptor Stimulation Brain Autonomic Nervous System Inhibited Sympathetic Activity Enhanced Parasympathetic Activity Heart Vessels Kidneys ↓ HR ↑ Vasodilation↓Stiffness ↑ Diuresis ↓ Renin secretion
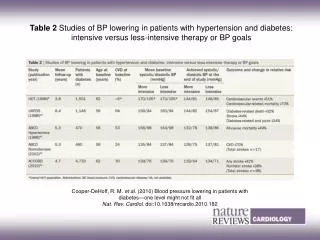
Prospective randomized double-blind trial 322 patients at 49 sites 55 roll-in patients / 265 randomized (2:1) Co-primary endpoints Short Term Acute Response Long Term Sustained Response Short Term Procedural AEs Short Term Hypertension Therapy AEs Long Term Device AEs Rheos Hypertension Pivotal Trial Design Implant Randomization 6-Month Blinded Evaluation Period 6-Month Blinded Evaluation Period Long-Term Follow-Up N = 181 Group A – Device ON Group A – Device ON N = 84 Group B – Device OFF Group B – Device ON -1 0 3 6 9 12 (months)
Key Inclusion Criteria SBP ≥ 160 mmHg DBP ≥ 80 mmHg 24 hour ABPM ≥ 135 mmHg At least one month of maximally tolerated therapy with at least three appropriate antihypertensive medications, including a diuretic
1st Endpoint – Short Term Acute Response20% super-superiority – Responder rate device ON vs. device OFF TRIAL ASSUMPTIONS TRIAL RESULTS 65% 70 N = 181 54% 60 N = 181 46% 45% 50 N = 84 A - B 40 % of Patients with ≥ 10mmHg SBP Reduction at 6 Months 30 20% Goal Diff (A-B) >20% N = 84 20 8% 10 0 Month-6 ON Month-6 OFF Month-6 ON - OFF
2nd Endpoint – Long-term Sustained ResponsePercent of Sustained Responders at 12 Months 100 90 88% 80 p-value < 0.001 % of Sustained Responders at 12 months 70 OPC: 65% 60 N = 97 Month-12 ON
3rd Endpoint – Short Term Procedure Adverse Events30-Day Event Free rate 90 • Types of Adverse Events • 4.4% permanent nerve injury (numbness, dysphagia, dysphonia) • 4.8% transient nerve injury • 4.4% general surgical complications (86% resolved) • 2.6% respiratory complaints (100% resolved) • 76% of all adverse events fully resolved OPC: 82% 80 75% 70 % of Patients Event Free at 30 days 60 50 N = 270 30-day Groups A+B
4th Endpoint – Short Term HTN Therapy Adverse Events6-Month Event Free Rate 100 91.7 87.6 90 15% + C.I. 80 72.6 Goal Diff (A-B) < 15% % of Patients Event Free at 6 Months 70 60 p-value < 0.001 N = 170 N= 85 Month-6 OFF Month-6 ON 40% Reduction of Hypertensive Crises, 23% Reduction of Events
5th Endpoint – Long Term Device Adverse Events12-Month Event Free Rate 100 p-value < 0.001 90 88% • Types of Adverse Events • 2% hypertension-related strokes • All other events < 2% • 76% of all adverse events fully resolved 80 % of Patients Event Free at 12 Months OPC: 72% 70 60 N = 265 12 Months Groups A+B
Endpoint Summary 7.7% 0% 20% 87.6 65% 100% 74.8 82% 100% 2.4% -15% 0% 87.2 72% 100%
Pre-Specified Ancillary Efficacy Analysis% of Patients at SBP ≤ 140mmHg p = 0.70 60 53% p = 0.005 51% N = 171 N = 81 45 42% N = 172 % of Patients SBP ≤ 140 mmHg 30 24% N = 80 15 0 Month-6 ON Group A Month-6 OFF Group B Month-12 ON Group A Month-12 ON Group B
Pre-specified Echo Sub-Study Long Term Regression in Left Ventricular Hypertrophy 120 117 p-value < 0.01 115 110 LV Mass Index (kg/m2) 105 102 100 95 N = 60 N = 60 90 12 Months Baseline
Additional Observations – Post-Hoc Efficacy AnalysisResults at 12 Months and Beyond 81% of patients were responders (SBP ≥ 10 mmHg relative to pre-implant) The average SBP drop at 12 months among responders was 44 mmHg 63% of responders reached blood pressure goal • Therapeutic efficacy continued to improve over time: 40 60% 54% 35 43% 30 26 45% SBP Reduction (mmHg) Percent Patients at SBP Goal 20 30% 10 15% 0 0 Month-6 ON Month-12 ON Month-6 ON Month-12 ON
Conclusions • 3 primary endpoints achieved: long term efficacy, long term device safety, and short term therapy safety • 2 primary endpoints not achieved: short term efficacy and procedure adverse events • Weight of overall evidence suggests long term efficacy of BAT to reduce blood pressure in resistant hypertension • These data justify further development of BAT
Moving Forward: Miniaturization to Reduce Procedure Invasiveness 1st Generation CSL New Generation CSL
Investigators and Participating Centers US Mark Passman; University of Alabama, AL Mason Weiss; Apex Cardiology Consultants, CA Fred Weaver; University of Southern California, CA Preston Flanigan; VISOC, CA Fadi Matar; Florida Cardiovascular Institute, FL Harischandra Karunaratne; Florida Hospital Cardiovascular Institute, FL Peter Wassmer; Heart & Vascular Institute, FL Jeffrey Travis; Southeast Regional Research Group, GA Michael Park; Iowa Heart Center, IA George Bakris; University of Chicago, IL Sibu Saha; University of Kentucky, KY Mitchell Weaver; Henry Ford Health System, MI Marcus Rothstein; Washington University, MO Paul van Bemmelen; Temple University, PA Gregory Roberts; Baptist Hospital of East Tennessee, TN Eric Peden; The Methodist Hospital System, TX Paul Kramer; Liberty Hospital, TX Stephen Motew; Novant Clinical research Inst, NC Vasilios Papademetriou; Veteran’s Affairs Medical Center, DC Branislav Schifferdecker; Oklahoma Cardiovascular Research, OK Gregory Trachiotis; GW Medical Faculty Associates, DC • James Fogartie; Rex HealthCare, NC • Deepak Gangahar; Nebraska Heart Institute, NE • Massimo Napolitano; Hackensack University Medical Center, NJ • Daichi Shimbo; Columbia University Medical Center, NY • John Bisognano; University of Rochester, NY • Anthony Comerota; Jobst Vascular Center, OH • Eugene Chung; The Lindner Clinical Trial Center, OH • Jean Starr; Ohio State University Medical Center, OH • Satish Muluk; Allegheny General hospital, PA • Paul Casale; Lancaster General Hospital, PA • William Todd Bohannon; Scott & White Memorial hosp, TX • William Edwards; St Thomas Research Institute, TN • James Hermiller; St Vincent Medical group, IN • Pat Kelly; Sanford research, SD • Michael Koren; jacksonville Center Clinical research, FL • Todd Reil; U of Minnesota, MN Europe • Peter De Leeuw; University of Maastricht, Netherlands • Hermann Haller; University of Hannover, Germany