Download
1 / 2
20 likes | 201 Vues
Relocation, relocation……learning through reflection C aroline Humphreys RGN Elaine Marriott RGN RSCN Polly Tarrant RGN.

E N D
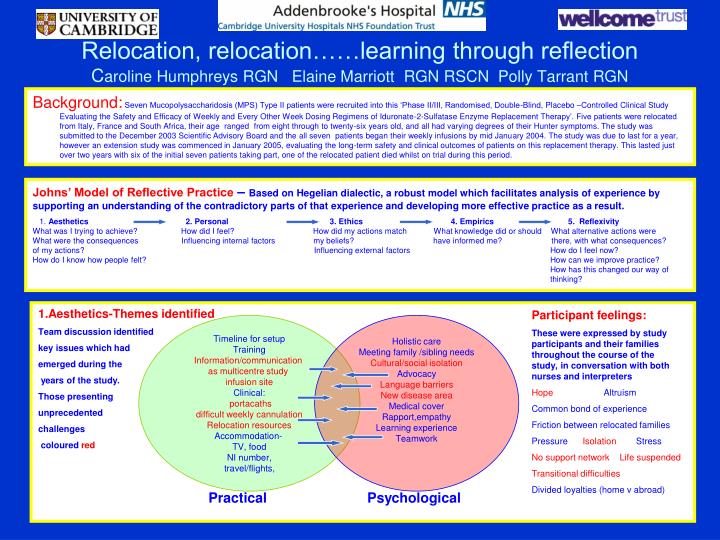
Relocation, relocation……learning through reflectionCaroline Humphreys RGN Elaine Marriott RGN RSCN Polly Tarrant RGN Background: Seven Mucopolysaccharidosis (MPS) Type II patients were recruited into this ‘Phase II/III, Randomised, Double-Blind, Placebo –Controlled Clinical Study Evaluating the Safety and Efficacy of Weekly and Every Other Week Dosing Regimens of Iduronate-2-Sulfatase Enzyme Replacement Therapy’. Five patients were relocated from Italy, France and South Africa, their age ranged from eight through to twenty-six years old, and all had varying degrees of their Hunter symptoms. The study was submitted to the December 2003 Scientific Advisory Board and the all seven patients began their weekly infusions by mid January 2004. The study was due to last for a year, however an extension study was commenced in January 2005, evaluating the long-term safety and clinical outcomes of patients on this replacement therapy. This lasted just over two years with six of the initial seven patients taking part, one of the relocated patient died whilst on trial during this period. Johns’ Model of Reflective Practice – Based on Hegelian dialectic, a robust model which facilitates analysis of experience by supporting an understanding of the contradictory parts of that experience and developing more effective practice as a result. 1. Aesthetics 2. Personal 3. Ethics 4. Empirics 5. Reflexivity What was I trying to achieve? How did I feel? How did my actions match What knowledge did or should What alternative actions were What were the consequences Influencing internal factors my beliefs? have informed me? there, with what consequences? of my actions? Influencing external factors How do I feel now? How do I know how people felt? How can we improve practice? How has this changed our way of thinking? 1.Aesthetics-Themes identified Team discussion identified key issues which had emerged during the years of the study. Those presenting unprecedented challenges colouredred Participant feelings: These were expressed by study participants and their families throughout the course of the study, in conversation with both nurses and interpreters Hope Altruism Common bond of experience Friction between relocated families Pressure Isolation Stress No support networkLife suspended Transitional difficulties Divided loyalties (home v abroad) Timeline for setup Training Information/communication as multicentre study infusion site Clinical: portacaths difficult weekly cannulation Relocation resources Accommodation- TV, food NI number, travel/flights, Holistic care Meeting family /sibling needs Cultural/social isolation Advocacy Language barriers New disease area Medical cover Rapport,empathy Learning experience Teamwork Practical Psychological
3.Ethics Where do our professional boundaries lie? Personal boundaries - how far to go? Group vulnerability through disease process Personal v professional issues in providing holistic care to family Did complacency associated with repetitive weekly visits diminish our focus? 2.Personal Feelings: Frustration, disappointment, excitement, hope, loss, failure, sadness, satisfaction, conflict Factors: Goalposts moving- whose benefit? participant/ doctor Transitional difficulties end of study Dealing with death Reciprocal expectations Lack of consistency of trials coordinator 4.Empirical Code of conduct Cultural awareness Respect Clarification of roles Advocacy Accountability Experience – or lack of? • 5.Reflexivity – implications for practice • Difficulty in knowing and observing professional and personal boundaries -open forums for exploration and discussion of issues arising, both practical and emotional. Refer back to Code of Conduct • Feeling of having to be ’all things to all people’ - Acknowledge limitations & work within role boundaries - Identify external resources and delegate ‘extended’ role – social services, MPS society • Lack of continuity of responsibilities – need firm, written agreement at outset regarding expectations and areas of responsibility, authority and accountability • Anticipation of cannulation difficulties on an ongoing basis due to nature of the disease and client group - stronger, earlier and robust advocacy for portacath insertion where appropriate • Making assumptions about participant & staff experience over long period of study - strong clinical leadership to maintain awareness, focus, skills • No experience of this type of study or disease area – not knowing what questions to ask -sharing of knowledge, experience and concerns, use of a competency framework to support staff and ensure expert practice • Lack of clarity of overlap between research and NHS treatment for research participants from abroad with different cultural expectations of health care – need to identify the issue and discuss with hospital management, sponsor and PI in advance of study onset References:Johns, C. (1995) Framing earning through reflection within Carper’s fundamental ways of knowing in nursing. Journal of Advanced Nursing, 22;226-234 Grech, E. (2004) Hegel’s Dialectic and Reflective Practice – a short essay. International Journal of Psychosocial Rehabilitation, 8, 71-73