Download
1 / 13

E N D
Investigation of the biliary tree • Ultrasound: stones & biliary dilatation • Plain radiograph: calcification • MRCP: anatomy & stones • Multi detector row computerised tomography scan: anatomy, liver, gall bladder and pancreas cancer • Radioisotope scanning: function • ERCP: anatomy, stones and biliary strictures • Percutaneoustranshepaticcholangiography: anatomy & biliary strictures • Endoscopic ultrasound: anatomy and stones
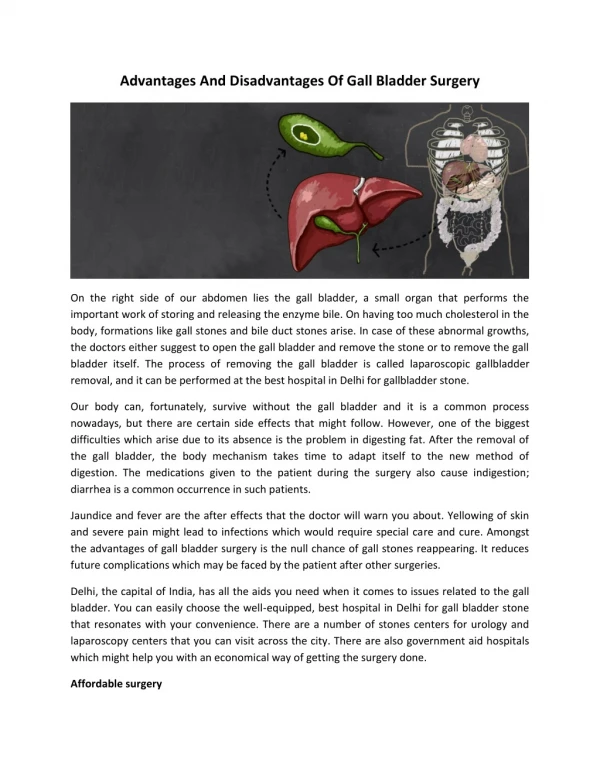
Effects and complications of gallstones • In the gallbladder • Biliary colic • Acute cholecystitis • Chronic cholecystitis • Empyemaof the gall bladder • Mucocele • Perforation • In the bile ducts • Biliary obstruction– obstructive jaundice • Acute cholangitis • Acute pancreatitis • In the intestine • Intestinal obstruction (gallstone ileus)
Differential diagnosis of cholecystitis • Common • Appendicitis • Perforated peptic ulcer • Acute pancreatitis • Uncommon • Acute pyelonephritis • Myocardial infarction • Pneumonia – right lower lobe • Ultrasound scan aids diagnosis • Uncertain diagnosis – do CT scan
Cholecystectomy: Preparation for operation • Full blood count • Renal profile and liver function tests • Prothrombintime • Chest X-ray and electrocardiogram (if over 45 years or medically indicated) • Antibiotic prophylaxis • Deep vein thrombosis prophylaxis • Informed consent
Post-cholecystectomy discomfort • If there is a delay in recovery after cholecystectomy, exclude bile duct or bowel injury • Incidence of bile duct injury is 0.05%
Indications for choledochotomy • Palpable stones in the common bile duct; • Jaundice, a history of jaundice or cholangitis; • A dilated common bile duct; • Abnormal liver function tests, in particular a raised alkaline phosphatase.
Causes of benign biliary stricture • Congenital • Biliary atresia • Bile duct injury at surgery • Cholecystectomy • Choledochotomy • Gastrectomy • Hepatic resection • Transplantation • Inflammatory • Stones • Cholangitis • Parasitic • Pancreatitis • Sclerosingcholangitis • Radiotherapy • Trauma • Idiopathic
Radiological investigation of biliary strictures • Ultrasonography • Cholangiographyvia T-tube, if present • ERCP • MRCP • PTC • Multidetectorrow CT
Bile duct cancer • Rare, but incidence increasing • Presents with jaundice and weight loss • Diagnosis by ultrasound and CT scanning • Jaundice relieved by stenting • Surgical excision possible in 5% • Prognosis poor – 90% mortality in 1 year
Gall bladder cancer • Rare • Presents as for benign biliary disease (gallstones) • Diagnosis by ultrasound and CT scanning • Excision in less than 10% – remainder palliative treatment • Prognosis poor – 95% mortality in 1 year
Reference • Bailey & Love-Short practice of Surgery.25th