Download
1 / 47
470 likes | 475 Vues
This article reviews the risk factors for neonatal and late onset hearing loss, provides recommendations for follow-up, and discusses ways to integrate risk factor conversation and tracking into practice.

E N D
Risk Factors for Late Onset Hearing Loss Betty Vohr MD AAP Representative to JCIH
2017 Universal Screening in US> 99% of Infants in the US have their hearing screenedNewborn screening identifies ~ 50% of HLFollow-up Rate for Pass with Risk Factors ?
Joint Committee on Infant HearingProgress and ChangeChallenge of Risk Factors for Hearing Loss
Objectives • Review risk factors for neonatal HL • Review risk factors associated with late onset HL & the recommended follow-up protocol • Describe ways to integrate risk factor conversation and tracking into practice
Why do we have late onset HL ? Recommendations for follow-up are based on the fact that standard NB screening does not identify all children who are deaf or hard of hearing because of missed mild or neural hearing loss, progressive hearing thresholds, and delayed- onset changes in hearing status The prevalence of children confirmed as deaf or hard of hearing neonates is 1.79/1000 school age is 3.65/1000
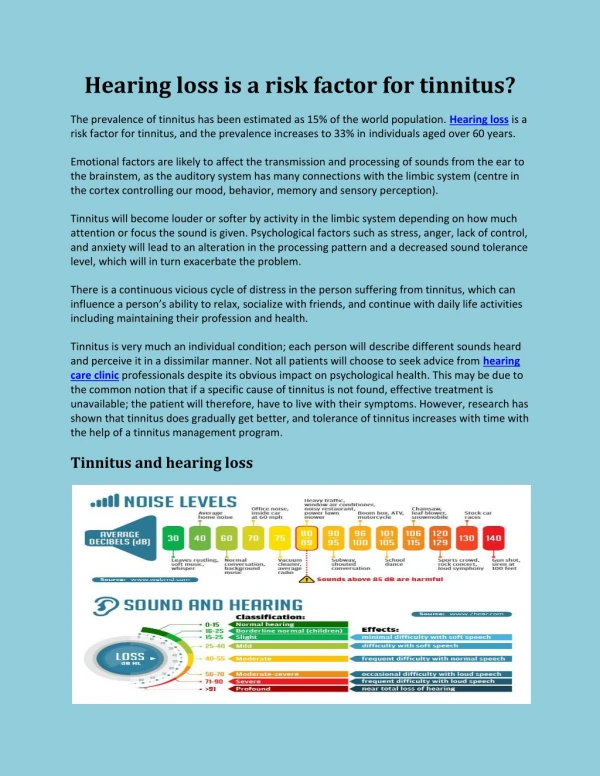
Range of Hearing • Normal 15-25 dB • Minimal 16-25 dB difficulty with soft sounds and noise • Mild HL 26-45 dB difficulty (soft speech & noise) • Mod HL 45-65 dB difficulty (conversational speech) • Sev HL 65-85 dB hear only loud speech or sounds • Prof HL > 85 dB no usable hearing
1 3 4-5
Risk Factor Changes • The prior eleven risk factors listed in JCIH 2017 are now listed as 12 separate factors and divided into subgroups of • predominantly “perinatal” (risk factors 1-9) and • “either perinatal or postnatal” (risk factors 10-12). • In addition, recommendations for follow-up and monitoring have been modified
First visit with parents: Time to start discussing language, HL and risk factors • In maternity Hospital or practice office • Have copy of discharge summary and hearing screen, risk results & risk factors for HL; discuss with family, query again re: risk factors • Enter all into EMR with prompts for all follow-up needed
Complete Medical Assessment • Timely medical assessment for all infants with suspected/confirmed mild, mod, severe, or profound levels completed no later than 3 m after diagnosis! Should be ASAP • Review detailed screening, dx, medical and family history • Comprehensive physical exam including middle ear, external changes, radiographic and lab studies consistent with best practices (AAP 2010)
Complete Medical Assessment • Refer: EI, ENT, Genetics, Ophthalmology minimum for infants who are confirmed as deaf/hard of hearing • Ophthalmology regularly • Additional providers as indicated clinically • Assess family needs and refer for support services as needed (counseling, social work, etc.) • Goal to provide optimal family centered care.
Script: Passed Newborn Screen; No Known Risk Factor First visit: Congratulations on the birth of your baby. The hearing screen was a pass. It is, however, important to monitor his/her speech and language development because hearing can change. Here is a brochure on speech and language development. We will review your infants development during your well child visits. Please let us know at any time if you have concerns. We can make a referral for further testing if needed.
Script: Passed Newborn Screen; Known Risk Factor First visit: • Congratulations on the birth of your baby. The hearing screen done in the hospital was a pass. • We have, however, identified that your baby has a risk factor for hearing loss. (> 5 days in NICU, VLBW, etc.) This means that your baby may be at ↑ risk of developing a hearing loss. • A follow-up hearing test is recommended in N months. We will continue to monitor your baby’s development. Please let us know at any time if you have concerns about your baby’s development. Here is a brochure about speech and language development. We can make a referral for further testing if needed.
Physical Exam • Growth Parameters • Microcephaly and/or short stature may suggest a congenital infection (e.g., CMV, rubella) or underlying genetic disorder. Tall, thin body habitus is associated with Marfan or Stickler syndrome. • Skin • Pigmentary abnormalities of skin and/or hair may signify a genetic syndrome associated with hearing impairment (cafe au lait macules in neurofibromatosis type 1, hypopigmented patches and/or white forelock in Waardenburg syndrome).
Physical Exam • HEENT • Assess for anatomic craniofacial abnormalities such as submucous cleft palate, pre-auricular tags/pits, auricular malformations. • Pneumatic otoscopy should be performed to assess tympanic membrane mobility and middle ear pressure. • Examine the neck (for masses), sinuses, and pits.
Physical Exam cont. • Extremities/Musculoskeletal • Musculoskeletal malformations may suggest a genetic syndrome associated with hearing impairment (e.g., cubitus valgus in Turner syndrome, fused digits in Apert syndrome). • Neurologic Exam • Abnormalities in tone or sensation may indicate an underlying neurologic disorder.
Routine blood testing of children with sensorineural hearing loss is of little diagnostic value and is not, consider obtaining a culture of saliva or urine for cytomegalovirus. Congenital progression therapy are evolving. CMV testing should be obtained prior to 3 weeks of age as those performed later cannot differentiate between congenital and postnatal infection. Postnatal infection is not associated with hearing loss. For more information, see CMV and Congenital Hearing Loss (UDOH) ( 648 KB) and Congenital Cytomegalovirus (CMV)-Related Hearing Loss. In older children, particularly those with a family history of renal failure, consider a urinalysis to assess for hematuria and proteinuria suggestive of Alport syndrome. Routine blood testing of children with sensorineural hearing loss is of little diagnostic value and is not recommended. [sensorineural hearing loss detected in the newborn period, consider obtaining a culture of saliva or urine for cytomegalovirus. Congenital CMV is a common cause of SNHL and antiviral treatment with valganciclovir may prevent progression of hearing impairment. The risks and benefits of antiviral therapy are evolving. CMV testing should be obtained prior to 3 weeks of age as those performed later cannot differentiate between congenital and postnatal infection. Postnatal infection is not associated with hearing loss. For more information, see CMV and Congenital Hearing Loss (UDOH) ( 648 KB) and Congenital Cytomegalovirus (CMV)-Related Hearing Loss. In older children, particularly those with a family history of renal failure, consider a urinalysis to assess for hematuria and proteinuria suggestive of Alport syndrome. Routine blood testing of children with sensorineural hearing loss is of little diagnostic value and is not recommended. [Mafong: 2002] For sensorineural hearing loss detected in the newborn period, consider obtaining a culture of saliva or urine for cytomegalovirus. Congenital CMV is a common cause of SNHL and antiviral treatment with valganciclovir may prevent progression of hearing impairment. The risks and benefits of antiviral therapy are evolving. CMV testing should be obtained prior to 3 weeks of age as those performed later cannot differentiate between congenital and postnatal infection. Postnatal infection is not associated with hearing loss. For more information, see CMV and Congenital Hearing Loss (UDOH) ( 648 KB) and Congenital Cytomegalovirus (CMV)-Related Hearing Loss. In older children, particularly those with a family history of renal failure, consider a urinalysis to assess for hematuria and proteinuria suggestive of Alport syndrome. Genetic Testing/ consultation • Genetic testing should be considered in all children without a known etiology for their HL. • Patients requiring genetic testing should be referred to a geneticist, genetic counselor, or interdisciplinary hearing assessment clinic, if available. • Genetic testing for commonly involved genes implicated HL is available and the cost is covered by insurance. • Connexin-26 mutations are the most common • Genetic testing will often predict which children need to be followed closely for retinal, renal, cardiac, etc. problems.
Causes of Permanent Hearing Loss in 100 Infants 40% Environmental 40 60% Genetic 60 30% syndromes (>400) 40 30% >75 genes ident 20 ½ are GJB2 – Connexin 26
Genetic Causes Single gene Connexin 26 Gene + environment Mitochondrial + ototoxic Gene + gene Gene + other gene
Genetic Causes of Hearing Loss: Contribution of Cx26 Genetic ~50-60% • 50% of DFNB - mutations of GJB2 or Connexin 26 • ~15% of congenital hearing loss – Cx26 mutations Syndromic ~30% Nonsyndromic ~70% Mt <1% Dominant 20% X-linked ~1% Recessive 80%
Routine blood testing of children with sensorineural hearing loss is of little diagnostic value and is not recommended. [Mafong: 2002] For sensorineural hearing loss detected in the newborn period, consider obtaining a culture of saliva or urine for cytomegalovirus. Congenital CMV is a common cause of SNHL and antiviral treatment with valganciclovir may prevent progression of hearing impairment. The risks and benefits of antiviral therapy are evolving. CMV testing should be obtained prior to 3 weeks of age as those performed later cannot differentiate between congenital and postnatal infection. Postnatal infection is not associated with hearing loss. For more information, see CMV and Congenital Hearing Loss (UDOH) ( 648 KB) and Congenital Cytomegalovirus (CMV)-Related Hearing Loss. In older children, particularly those with a family history of renal failure, consider a urinalysis to assess for hematuria and proteinuria suggestive of Alport syndrome. Routine blood testing of children with sensorineural hearing loss is of little diagnostic value and is not recommended. [Mafong: 2002] For sensorineural hearing loss detected in the newborn period, consider obtaining a culture of saliva or urine for cytomegalovirus. Congenital CMV is a common cause of SNHL and antiviral treatment with valganciclovir may prevent progression of hearing impairment. The risks and benefits of antiviral therapy are evolving. CMV testing should be obtained prior to 3 weeks of age as those performed later cannot differentiate between congenital and postnatal infection. Postnatal infection is not associated with hearing loss. For more information, see CMV and Congenital Hearing Loss (UDOH) ( 648 KB) and Congenital Cytomegalovirus (CMV)-Related Hearing Loss. In older children, particularly those with a family history of renal failure, consider a urinalysis to assess for hematuria and proteinuria suggestive of Alport syndrome. Laboratory testing • Dx in first 2 weeks- culture of saliva or urine for CMV • In older children with hx of renal disease ; urinalysis for hematuria and proteinuria suggestive of Alport Syndrome
Other Testing • Electrocardiography is indicated if there is a family history of prolonged QT interval or sudden death, or if medical history is significant for syncope, arrhythmia, or history of ALTE. • An ECG should also be considered in all infants with severe-profound sensorineural hearing loss of unknown etiology.
Referral to Pediatric Otolarygology • Performs a comprehensive evaluation of the head and neck and can help in the identification of craniofacial malformations associated with hearing loss. • Should work closely with the audiology team (including Early Intervention specialist) to determine intervention planning for hearing loss. • Performs surgical intervention if necessary (e.g., tympanostomy tubes, reconstruction, cochlear implant, bone-anchored hearing aids).
Pediatric Ophthalmology • Every child with confirmed permanent HL should undergo annual evaluation by an ophthalmologist to determine visual acuity and evaluate for concomitant vision disorders (e.g., Usher Syndrome, cataracts ).
Summarizes the Medical Work-up • Physical exam • Skin dysplasia, or atresia, craniofacial abnormalities, skeletal abnormalities • Dysmorphism • MEE • Family History of HL onset <30 years • History of care in NICU for > 5 days • Urine Culture for CMV- most common infectious cause • CT of inner ear to r/o anatomic abnormalities • Genetic studies to r/o Connexin 26 and 30/other • EKG for severe/profound to r/o long QT Syndrome • Consults with otolaryngology, genetics, and ophthalmology
New Protocol in WBN • Well-babies screened and not passed by AABR may be rescreened and passed by OAE; The WBN rate of AN < 1%. • Although there is a possibility of missing AN, there is an unacceptable high “loss-to-follow-up” rate for infants who do not pass the birth screen and fail to return for rescreening. • The revised recommendation is that WBN screen and second in-hospital screen may use either OAE or AABR. • However, the recommendation to rescreen using only AABR for the infant who does not pass initial AABR continues to be the Committee’s preferred protocol
EHDI A reconsideration for 1-3-6 m screening completed by 1 m, audiologic diagnosis by 3 m, enrollment in Early Intervention by 6 m be updated to the recommendation of 1-2-3 m • Earliest age of identification is encouraged to provide audiologic testing in natural sleep and to facilitate early access to language
Surveillance in the Medical Home • All infants should have regular surveillanceby their PCP consistent with the pediatric periodicity schedule of: • auditory skills • developmental milestones • parent concerns regarding hearing or language • middle ear effusion
Outpatient Rescreening • Rescreening should comprise a single rescreen of both ears in the same session, regardless of initial screening results • There is an obligation to report outcomes of all rescreen results whether passed or not passed, to the state EHDI • The JCIH supports the AAP published guidelines for rescreening in the Medical Home ( AAP, 2014)
Equipment • Ensure initial equipment calibration is performed by a manufacturer or distributor in a manner consistent with purported screening parameters • Oversight to ensure equipment parameters remain appropriate. • Requirements for troubleshooting, annual calibration, and expected performance should be reviewed by the audiologist. .
Rescreening in the Medical Home • Rescreen must be performed using an automated physiologic device (OAE or AABR) - Not behavioral (whisper, rattle, other noises) • Equipment must be calibrated initially and annually by manufacturer or hospital engineering dept. • Must have quiet environment & appropriately trained personnel • Always rescreen both ears • Report outcomes of all rescreen results whether passed or not passed, to the state EHDI
Rescreening in the Medical Home Exception to Medical Home Rescreening: • NICU infants who do not pass hospital screen should always be referred directly to audiology
Surveilance/Screening in the Medical Home • All infants should have an objective standardized screen of global development with a validated tool at 9, 18, and 24-30 months of age. ( i.e. Ages and Stages) • Children who do not pass a medical home global screen or if there is concern regarding hearing or language should be referred for speech-language evaluation and audiology assessment.
Clinical signs of possible hearing loss • Irritability, inattention, behavior problems • Delayed speech and language skills • Unintelligible speech • Child only responds when signal is loud or when in a quiet room • Uncharacteristic voice pattern- low and unmodulated • Child turns TV on very loud
Vital Records and Newborn Developmental Risk Assessment Newborn Blood Spot KIDSNET Home Visiting LeadPrevention Pediatricians Audiologists EarlyIntervention Rhode Island Department of Health RI Hearing AssessmentProgram WIC: Special Supplemental Nutrition Program for Women, Infants and Children Birth Defects Immunizations Head Start School Nurses
Resources for the Medical Home • www.babyhearing.org Great for parents • www.infanthearing.org • http://www.ncbi.nlm.nih.gov/books/NBK1434/ • Hands and Voices www.handsandvoices.org • Boystown National Research Hospital research and videos • https://www.cdc.gov/ncbddd/hearingloss/genetics.html • American sign language www.nidcd.nih.gov
For Infants and young Children there should always be Urgency for Diagnosis and Intervention for HL to ensure the best outcome
Thank You Questions ?