Download
1 / 8
100 likes | 738 Vues
Low Vision Services. Jenny Lindsay Co-Deputy Head of Optometry Belfast Health and Social Care Trust. Definitions.

E N D
Low Vision Services Jenny Lindsay Co-Deputy Head of Optometry Belfast Health and Social Care Trust
Definitions • A person with low vision is one who has an impairment of visual function for whom full remediation is not possible by conventional spectacles, contact lenses or medical intervention and which causes restriction in that person's everyday life. • A low vision service is a rehabilitative or habilitative process, which provides a range of services for people with low vision to enable them to make use of their eyesight to achieve maximum potential. • (Low Vision Services Consensus Group Document, 1999)
Epidemiology • N. Ireland has an ageing population • Visual impairment increases with age • 0-15yrs, 7/100,000 population reg B or PS • 75-84yrs, 431/100,000 population reg B or PS • 85+yrs, 946/100,000 population reg B or PS (Evans et al, 1995 and 1996) • 48 000 people with visual impairment in N. Ireland (NISRA)
Standards 1 (DOH, 2007) • Multi-disciplinary, multi-agency approach (health, social care and voluntary providers) • Flexible and able to meet the needs of those with additional disabilities e.g. learning disabilities • Accessible (referral and location) • Personnel suitably trained or undergo training programme leading to accreditation • Service improvement, monitoring and evaluation of the service – include user opinions
Standards 2 (DOH, 2007) • Comprehensive range of services – • Functional visual assessment • Range of optical, non-optical and electronic aids available • Training and/or therapy • Links to other services (home assessment and mobility, education and employment services) • Access to support, advice and counselling
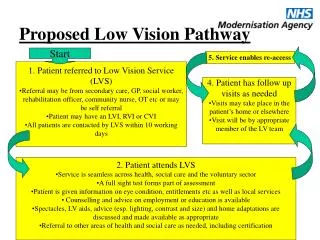
Service models • “Traditional” hospital optometry low vision clinic • “One stop shop” e.g. Birmingham Focus, RNIB Judd Street, Gateshead • Community model e.g. Welsh Low Vision Scheme • Main advantage is ease of access • More challenging cases difficult to manage • Initial set-up and accreditation • To date no reliable research to compare outcomes or cost-effectiveness with different models
Northern Ireland • 2 bases Royal Victoria Hospital and Altnagelvin Area Hospital • Outreach services at 12 other locations throughout N. Ireland • Weekly clinic at University of Ulster, Coleraine • Joint optometric and rehabilitation assessments • Wide range of visual function tests and low vision aids • 67% of LVAs loaned at initial appointments are illuminated stand magnifiers and 63% ≤x5 magnification (Lindsay et al, 2004)
Benefits and Challenges • 69% use LVAs regularly, 96% benefited from rehab support and 96% overall reported benefit from attending the LVC (Lindsay et al, 2004) • Number of LVC appointments risen from 2500 to 5000 in last 10 years • Waiting times 6 months in some locations • Future – do we extend current service or look at alternative ways of providing low vision services?