Download
1 / 24
320 likes | 576 Vues
Bronchiolitis and Synagis. Pretest . Which of the following children should receive RSV prophylaxis during RSV season? A. 5 month former 34 weeker who attends day care and has a 5 yo brother B. 11 month former 27 weeker C. 7 month former 31 weeker

E N D
Pretest • Which of the following children should receive RSV prophylaxis during RSV season? A. 5 month former 34 weeker who attends day care and has a 5 yo brother B. 11 month former 27 weeker C. 7 month former 31 weeker D. 18 month patient with cystic fibrosis on home 02 E. 14 month Tetrology of Fallot patient F. 22 month former 32 weeker with BPD who required diuretics and steroids in October
Background • Respiratory syncytial virus (RSV) is the primary cause of lower respiratory tract illness in young children. • Generally resolves uneventfully in otherwise healthy children. • High risk populations may develop severe and sometimes fatal lower respiratory tract infections. : )
Background • RSV infection annually contributes up to 126,300 pediatric hospitalizations in the U.S. • Estimated annual hospitalization costs for RSV pneumonia in children <=4 years: $300 - $400 million (1998 $), now much greater. • Annual mortality due to RSV in infants and children is estimated to range from 200 to over 2,700.
Microbiology Basics • RSV is single-stranded RNA virus of Paramyxoviridae family • Two subtypes, A and B • A subtypes cause more disease • Within subtypes are several genotypes • Strains have shifts each year, accounting for re-infections
Prematurity • Prematurity increases risk of severe RSV infection. RSV Hospitalization Rate by Gestational Age at Birth
Epidemiology • Worldwide RSV epidemics occur yearly • United States: November – April • Peak: January – March (most areas) • Peak: 2 – 3 months earlier (Southeast) • 80% RSV admissions occur within 4 months of discharge from NICU. Respiratory Illness Hospitalization Rate by Month of Discharge from NICU in Infants <= 32 Weeks GA
Transmission • Inoculation of nasal or ocular membranes after contact with virus containing secretions or fomites • Virus can survive for several hours on hands and fomites (WASH HANDS!!!) • Direct contact most common, large aerosol drops also implicated • Incubation is 2-8 days • Patients usually shed 3-8 days but can shed up to 4 weeks in young infants
Immunity • Almost everyone has been infected with RSV by age 3 • Does not convey total protection against reinfection • Can be infected more than once in same RSV season but usually 2d infection milder • Transplacental Ab does not protect completely against infection but high Ab’s imply milder disease and usually is only in upper respiratory tract
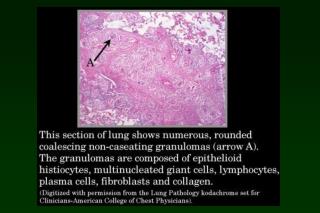
Pathologic findings • Necrosis of epithelial cells • Proliferation of bronchiolar epithelium • Infiltrates of monocytes and T cells around arterioles • Neutrophils between vasculature and small airways • Leads to airway obstruction, air trapping, increased airway resistance • Increased incidence of wheezing as children grow older
Hospital therapy for RSV • Care is mainly supportive (fluids, respiratory support) • Trial (one dose) of beta-agonist if bronchospasm. D/C if not improvement • Steroids not recommended • Ribavirin not recommended unless severe LRT infection • Neither RSVIG nor Synagis is effective in treatment of hospitalized children
RSVIG • Was developed as hyperimmune globulin from donors with high titers of RSV antibody • In trials reduced hospitalizations in high risk infants by 41-63% • Increased morbidity and mortality in CHD patients • Interfered with immune response to live vaccines (MMR and varicella) • No longer used frequently
Palivizumab (Synagis) • Is monoclonal antibody (not blood product) against RSV F glycoprotein • Easier to administer than RSVIG • Does not interfere with response to live vaccines • A newer but similar product is MEDI-524 or Numax • More potent in animal trials • Currently undergoing clinical evaluation
Synagis • Synagis is available in 50 and 100 mg vials • The cost is $725 per 50 mg and $1370 per 100 mg vial • Synagis has a shelf life of 6 hours making drug wastage nearly inevitable
Dosing of Synagis • 15 mg/kg IM once per month for 5 doses • Begin before RSV season begins, October or November • Once dosing begins, continue even if patient is past age of indication • Continue even if breakthrough infection
Efficacy • IMpact-RSV trial in BPD pts and preemies • 55% reduction in RSV-associated hospitalizations vs placebo • Trial in CHD pts • 45% fewer hospitalizations • 73% fewer hospital days needing O2 • 56% fewer total hospital days • Trial in 421 preemies without CLD who received Synagis or placebo • 50% fewer infants in Synagis group had recurrent wheezing • Shows that prevention of RSV LRTI may reduce risk of recurrent wheezing in preemies without CLD
Risk factors for severe disease • Less than 6 months • Born during first half of RSV season • Attending daycare • Underlying lung disease • Born before 35 weeks • Congenital heart disease • Immunocompromised patients • SCIDS, leukemia, BM transplant • Significant asthma (any age) • Living at altitudes greater than 8000 feet • Institutionalized elderly
Adverse Reactions • Extremely safe, no serious adverse events in two consecutive seasons seen • Severe hypersensitivity (less than 1 per 100,000) • About 1 per 100 children will have anti-Synagis antibodies and antibody response declines with continued dosing • No resistance to Synagis by RSV seen • Doesn’t interfere with immunizations
Specific Recommendations • BPD- younger than 2 yo needing medical therapy for lungs who required medical therapy within 6 mos of RSV season • CHD – under 2 who have hemodynamically significant CHD • Prematurity • ≤ 28 weeks, younger than 1 yr at start of season • 29-35 wks, younger than 6 mos • 32-35 consider for infants <6 mos if 2 risk factors (day care attendance, congenital abnormalities, NMD, school-aged sibs) • Immunocompromised – no controlled studies but seems apparent that those with SCIDS or HIV with low CD4 undergoing chemotherapy or post-transplant would benefit • Structural or functional lung disease (such as CF) are at increased risk; no data on effectiveness
Medicaid and Synagis • Synagis is a benefit under the Comprehensive Care Program • Administered by a Synagis provider • Eligibility for children under 2 the same except: • Hemodynamically significant heart disease is defined as including: • Pulmonary hypertension • Digoxin or diuretics • Oxygen • Lung disease qualifies if: • On steroids, diuretics, ventilator or 02 • Transplants patients qualify
RSV Vaccine • Many challenges for effective vaccine • Immature immunity • Possible suppression of immune response by maternal antibody • Several antigenically divergent strains • Live attenuated vaccines are being tested • Must be very attenuated in this young group • However, lessens chance of detectable Ab response
Post-test • Which of the following children should receive RSV prophylaxis during RSV season? A. 5 month former 34 weeker who attends day care and has a 5 yo brother B. 11 month former 27 weeker C. 7 month former 31 weeker D. 18 month patient with cystic fibrosis on home 02 E. 14 month Tetrology of Fallot patient F. 22 month former 32 weeker with BPD who was required diuretics and steroids in October
Answer to Pretest Question There is evidence for lack of benefit in the 7 month old 31 weeker No evidence for benefit in cystic fibrosis patient but is reasonable to consider
References • Up To Date, “Treatment and Prevention of RSV” • AAP Clinical Practice Guidelines, “Diagnosis and Management of Bronchiolitis”, PEDIATRICS Volume 118, Number 4, October 2006 • AAP Policy Statement, Revised Indications for the Use of Palivizumab and Respiratory Syncytial Virus Immune Globulin Intravenous for the Prevention of Respiratory Syncytial Virus Infections