Download
1 / 46
460 likes | 836 Vues
Behandling af motoriske komplikationer ved Parkinsons sygdom med DBS, Apomorphin og Duo- dopa. 2010.

E N D
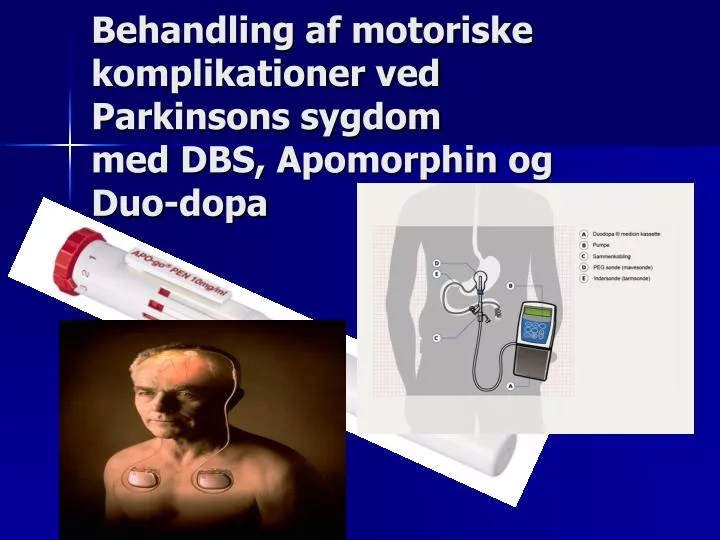
Behandling af motoriske komplikationer ved Parkinsons sygdom med DBS, Apomorphin og Duo-dopa 2010
Komplikationer Melamed E. Mov Disord 2007;22 suppl17:S37-84; Bhidayasiri R. J Neurol Sci 2008;266(1-2):204-15.Antonini A. Parkinsonism Relat Disord 2007;13suppl:S24-8. Widnell K. Mov Disord 2005; 20 suppl11:S17-22 • Motoriske fluktuationer Wearing off On-off-fænomener Freezing • Dyskinesier • Synshallucinationer og andre psykotiske symptomer
“on” timewith Dyskinesia 3.5 hours (20%) “on” time 5.6 hours (32%) 8.4 hours (48%) “off” time Wake-up Time 5.30 hours Time of Day Bed Time 24.00 hours “on” timewith Dyskinesia 3.5 hours (20%) “on” time 5.6 hours (32%) “off” time 8.4 hours (48%) e Wake-up Time 5.30 hours Time of Day Bed Time 24.00 hours MOTORISKE KOMPLIKATIONER Karen Østergaard, professor, overlæge dr.med., Neurologisk afd., Aarhus Universitetshospital
Deep Brain StimulationTargets • Parkinsons sygdom (STN) • Tremor (VIM) • Dystoni (GPi)
Deep Brain Stimulation (DBS) • Stereotactically placed into target nucleus • High frequency, pulsatile, bipolar electrical stimulation • Can be activated and deactivated with an external magnet/computer • Exact physiology unknown, higher frequencies mimic cellular ablation, not stimulation
Functional subdivisions of the primate STN:the dorsolateral somatomotor part (blue), the ventromediallyassociative part (green) and the medial limbic part (red)Temel Y et al. Progress in Neurobiology 2005; 76:393
DBS mekanismeHammond C. Movement Disorders 2008; published online sep 10; Vitek JL. Cleveland Clinic Journal of Mediicne. 2008;75 suppl 2: S59-65, • High frequency stimulation interfererer med spontane patologiske mønstre ved at introducere normal aktivitet i adskillige “knudepunkter” i det neurale netværk • It seems that decrease of low-frequency beta oscillations (11-30 Hz) in the basal ganglia • And generation of gamma frequencies (30-80 Hz) may be required to initiate locomotion and improve PD symptoms
Patient selektion til STN DBSBenabid et al. Deep Brain stimulation of the subthalamic nucleus for Parkinsons disease: methodological aspects and clinical criteria. Neurology 2000; 55: S40-S44. Indikation: • Bilateral idiopatisk Parkinsons sygdom (PS) • Motoriske komplikationer til levodopa behandling (on-off fænomener og/eller dyskinesier) og/eller svær tremor • Yderligere forbedring kan ikke opnås ved optimering af den medicinske behandling • Alder 30-65 (70) år • Patienten må ikke have anden betydende medicinsk sygdom, som ikke er velkontrolleret • Patienten må ikke have betydende neuropsykiatriske symptomer
Forudsætninger vedr. motoriske forhold • Levodopa responsiv PS • UPDRS III >30 efter 12 timers pause med parkinson medicin (praktisk defineret off) • Hoehn and Yahr stadium 3-4 (5) i off tilstand • Levodopa responsiv PS dvs. min 30% forbedring af UPDRS III efter indtagelse af en sufficient levodopa dosis
Forudsætninger vedr. intellekt og psyke • Patienten må ikke være dement • Patienten må ikke have svær eller intraktabel depression • Forsigtighed ved tidligere suicidal forsøg • Patienten må ikke have vedvarende psykiatriske symptomer herunder adfærdsforstyrrelser • Ardouin et al. Bilateral subthalamic or pallidal stimulation for Parkinson's disease affects neither memory nor executive functions: a consecutive series of 62 patients. Ann Neurol 1999; 46: 217-23.
RESULTS FOR 26 PATIENTS1 YEAR AFTER SURGERY • MEAN AGE 59 YEARS • GENDER 21M/5F • MEAN DURATION OF DISEASE 15 YEARS • The Deep-Brain Stimulation for Parkinson’s Disease Study Group. Deep-brain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus in Parkinson’s disease. N Engl J Med 2001; 345: 956-963. • Ostergaard K, Sunde Naa, Dupont E. Effects of bilateral stimulation of the subthalamic nucleus in patients with severe Parkinson's disease and motor fluctuations. Mov Disord 2002; 17: 693-700.
Bivirkninger/komplikationer. • Operative komplikationer: hemorrhagi, infektion • Komplikationer/bivirkninger relateret til stimulationen: dysarthri, forværring af gang- og balance, dysphagi, dobbeltsyn, øjenlågsapraksi, dystoni, dyskinesier • Komplikationer relateret til udstyret: elektrode displacering, kabelbrud, tekniske komplikationer • Vesper J, Chabardes S, Fraix V, Sunde N Aa, Østergaard K. Dual Channel Deep Brain Stimulation system for Parkinson’s Disease and Essential Tremor - A prospective multi-center open label clinical study. J Neurol Neurosurg Psychiatry 2002; 73:275-280.
Bivirkninger/komplikationer • Forbigående postoperative psykiske komplikationer: konfusion, hallucinationer, mani, psykotiske episoder, depression • Vedvarende postoperative psykiske komplikationer: psykose, adfærdsmæssige forstyrrelser, apati, depression, suicidium, demens • Houeto et al. Behavioral disorders, Parkinson's disease, and subthalamic stimulation. J NNP 2002; 72: 701-707 • Jahanshahi M, Ardouin C M et al. The impact of deep brain stimulation on executive function in Parkinson's disease. Brain 2000; 123: 1142-54. • Saint-Cyr JA, Trepanier LL et al. Neuropsychological consequences of chronic bilateral stimulation of the subthalamic nucleus in Parkinson's disease. Brain 2000; 123: 2091-108.
Forbedring af patientens livskvalitet • Efter 6 måneders behandling med STN stimulation: significant forbedring af mobilitet, ADL og cognition. Kontrolgruppen opnåede ikke nogen forbedring i livskvalitet målt med PDQ-39. • Just H and Ostergaard K. Health-Related quality of life in patients with advanced Parkinson's disease treated with deep brain stimulation of the subthalamic nuclei. Mov Disord 2002; 17: 539-45. • Martinez-Martin P, Valldeoriola F, Tolosa E, Pilleri M, Molinuevo JL, Rumia J, Ferrer E. Bilateral subthalamic nucleus stimulation and quality of life in advanced Parkinson's disease. Mov Disord 2002; 17: 372-7. • Deuschl G et al. A randomized trial of DBS for PD. New Engl J Med 2006;355:896
Teamfunktion • Et godt behandlingsresultat forudsætter teamfunktion: • Neurokirurg, neurolog, neuroradiolog, neuropsykolog, talepædagog, sygeplejerske, fysioterapeut • Houeto JL, Damier P, Bejjani PB et al. Subthalamic stimulation in Parkinsons disease: a multidisciplinary approach. Arch Neurol 2000; 57: 461-465.
Langtids resultater • Author Year N Years Motor ADL Dysk Off Med • Krack 03 42 5 54(off) 49(off) 72 64 • Rodrig. 04 10 4 71(on) 61(on) 53 50 -Oroz • Osterg. 06 22 4 55(off) 42(off) 90 67 29
Parkinson´s disease DBS STN 5 year results (Krack. NEJM 2003;349:1925-34) (Østergaard and Sunde Mov Disord 2006;21:624) • On-medication compared with 1-year results • Akinesia and speech and post.stab. and gait worsened, • Painful off-period dystonia disappeared in most patients • The deterioration in axial symptoms is consistent with the natural history of the disease
Parkinson´s disease DBS STN 5 year results(Krack. NEJM 2003;349:1925-34) • 5-years after surgery and off-medication most patients were independent in ADL • Before all depended on a caregiver • Stimulation parameters and medication was kept constant from 1 to 5 years in other words tolerance to stimulation did not develop
Konklusion: hvilke patienter vil have mest gavn af DBS i STN? • Yngre < 65 år (70 år) • Med motoriske fluktuationer og/eller svær tremor • Ikke-demente og psykisk stabile uden betydende adfærdsforstyrrelser og med et velfungerende familieliv/omgangskreds
Konklusion: hvilke patienter vil have mindre gavn af DBS i STN? • Ældre > (65) 70 år • Med levodopa resistent svær dysarthri • Udtalte gang-og balanceforstyrrelser i on fase • Begyndende demens
Treatment of tremor with DBS • Essentiel tremor, bilateral DBS of the VIM nucleus • Development of tolerance • Development of dysarthria and postural instability • Alternative treatment: unilat. DBS of VIM • Parkinson tremor, bilateral DBS of the VIM nucleus (80% reduction in contralateral arm and leg tremor) • Risk that rigidity and bradykinesia become more prominent • why bilateral STN stimulation is preferred • Risk of postural instability and dysarthria • Alternative treatment: unilat. DBS of VIM • Alternative treatment: unilat. DBS of STN • Holmes tremor • Bilateral DBS of the VIM nucleus
Conclusion • Selection of patients, include the family • Adverse events • Serious complications, are the risks warranted by the results • Long-term effect and complications • Team function • Follow-up, life-long
Apomorfin behandling ved PSScndinavian consensus based on Movement Disorder Conference in Bremen 2007 • Farmakokinetik • Skal gives parenteralt, inaktiveres i leveren efter peroral indgift • Virkningen indtræder 7-8 min efter s.c. indgift • Virkningsvarigheden er ca. 60 min. efter en enkelt injektion • Kan gives s.c. som injektioner eller kontinuerligt via pumpe
Indikation for behandling med Apomorfin ved PSScndinavian consensus based on Movement Disorder Conference in Bremen 2007 • Indikation • Betydende off-perioder på trods af optimal peroral medicinsk behandling • Forudsætning • God l-dopa eller apomorfin respons • Patient og/eller caregiver skal være i stand til at forstå og udføre behandlingen • Er der brug for mere end 6-(10) daglige inj. overvejes apomorfin pumpe behandling • Uddannet PS sygeplejerske
Apomorfin behandling: Eksklusion Scandinavian consensus based on Movement Disorder Conference in Bremen 2007 • Apomorfinintolerans • Udtalte dyskinesier • Udtalt ortostatisme • Ikke behandlet snævervinklet glaucom • Depression • Hallucinationer og andre psykotiske bivirkninger, hypomani • Demens • Dopamindysregulations syndrom • Betydende cardiovaskulær sygdom, respiratoriske sygdom, nyre- og lever-insufficiens • Graviditet og amning
Apomorfin behandlingsstart • Domperidon 20 mg x 3 i 2-3 dage inden start på behandling og i den første tid. Kan evt. senere aftrappes • Coombs test før og hver 6:måned • Apomorfin test for at undersøge effekt og bivirkninger • Anvend lavest dosis som giver tilfredsstillende effekt • Instrueres i genkendelse af første tegn på off-symptomer
Apomorfin behandlingsstart • Reducer sædvanlig parkinson medicin 50% • Pumpe infusion startes med 1mg/time og øges med 0,5-1 mg/time og dag
Apomorfin test • Fastlæggelse af dosis sker i off-tilstand efter 12 timers pause med parkinsonmed. • Initialt 1 mg s.c. Hvis der ikke er opnået tilfredsst. reaktion efter 30 min., gives 2 mg s.c. • Dosis øges trinvis med mindst 40 minutters interval, indtil tilfredsst. motorisk reaktion er opnået (tærskelværdi). • Den daglige dosis kan derefter gives som 1-6 injektioner, højst 7 mg som enkeltdosis. • Er der brug for 6-10 daglige injektioner eller mere end 30 mg/dag, overvejes at give apomorphin som kontinuerlig s.c. infusion ved hjælp af elektronisk justerbar pumpe.
Apomorfin behandling bivirkninger • Hæmolytisk anæmi (3%), eosinophili • Kvalme, opkastning, svimmelhed • Ortostatisme • Somnolens, træthed, konfusion • Hallucinationer, psykotiske symptomer
Som ovenfor Lokale noduli på infusionsstedet Nyt infusionssted hver dag Max koncentration af apomorfirn er 5 mg/ml Apomorfin bivirkninger
Apomorfin referencer • 1. Hagell P, Odin P. Apomorphine in the treatment of Parkinson´s disease. J Neurosci Nurs 2001;33:21-38 • 2. Kolls BJ, Stacy M. Apomorphine: a rapid rescue agent for the management of motor fluctuations in advanced Parkinson disease. Clin Neuropharmacol 2006;29:292-301 • 3. Obering CD, Chen JJ, Swope DM. Update on apomorphine for the rapid treatment of hypomobility („off“) episodes in Parkinson´s disease. Pharmacotherapy 2006;26:840-52
Apomorfin referencer • 6. Dewey RB, Hutton T, LeWitt A et al. A randomized, double-blind, placebo-controlled trial of subcutaneously injected Apomorphine for parkinsonian off-state events. Arch Neurol 2001;58:1385-92 Evidence Level: Ib • 7. Pahwa R, Koller WC, Trosch RM, Sherry JH; APO303 Study Investigators. Subcutaneous apomorphine in patients with advanced Parkinson's disease: a dose-escalation study with randomized, double-blind, placebo-controlled crossover evaluation of a single dose. J Neurol Sci. 2007 Jul 15;258(1-2):137-43. Epub 2007 Apr 27 Evidence Level: Ib • 8. Pfeiffer RF, Gutmann L, Hull KL Jr, Bottini PB, Sherry JH; APO302 Study Investigators. Continued efficacy and safety of subcutaneous apomorphine in patients with advanced Parkinson's disease. Parkinsonism Relat Disord. 2007 Mar;13(2):93-100. Epub 2006 Oct 18 Evidence Level: Ib
Behandling med Duodopa • Indikation • Behandling af svær PS med motoriske fluktuationer og/eller dyskinesier på trods af optimal peroral behandling • Forudsætning • L-dopa respons • Uddannet PS sygeplejerske • Administration • Enteralgel. 1 ml indeholder 5 mg carbidopa og 20 mg levodopa. • Beregnet til enteral administration ved hjælp af elektronisk pumpe og permanent sonde i duodenum via perkutan endoskopisk gastrostomi (PEG). • Initial behandling og indstilling af dosis via nasoduodenal sonde.
Initial behandling og indstilling af dosis via nasoduodenal sonde
Enteral administration ved hjælp af elektronisk pumpe og permanent sonde i duodenum via perkutan endoskopisk gastrostomi (PEG).
Duodopa kontraindikationer • Allergi overfor levodopa eller carbidopa • Ubehandlet snæver vinklet glaucom • Svær lever eller nyre sygdom, svær hjerte inkompensation, betydende hjerte arytmier, nylig apoplexi, • Pheochromocytom, hyperthyroidisme, Cushings syndrom • Kontraindikationer mod abdominal kirurgi • Betydende demens • Behandling med uselektiv MAO hæmmer eller MAO-A hæmmer
Duodopa • Dosis udregnes på basis af tidligere oral levodopa behandling og behandling med dopamin agonister • Omregnes til levodopa ækvivalente doser • Vedligeholdelsesdosis. Individuelt, sædvanligvis 40-120 mg levodopa/time i 16 timer, bør holdes inden for 20-200 mg/time.Voksne. Morgenbolusdosis. Sædvanligvis 100-200 mg levodopa, højst 300 mg som bolus. Ekstra bolusdosis 10-40 mg levodopa efter behov. Hvis behovet for ekstra doser overstiger 5 gange pr. dag, bør vedligeholdelsesdosis forhøjes. • Som regel som monoterapi • Evt. dosis af dopamin agonist til natten
Komplikationer • Infektion omkring sonden, peritonitis • Hypertrofisk granulationsvæv omkring sonden • Displacering af sonden op i ventriklen • Kateter knæk eller blokade • Kateter afkobling
Referencer • Kurth MC, Tetrud JW, Tanner CM, et al. Double-blind, placebo-controlled, crossover study of duodenal infusion of levodopa/carbidopa in Parkinson’s disease patients with “on-off” fluctuations. Neurology 1993;43:1698-1703. • Evidence Level: Ib • Nyholm D, Nilsson Remahl AI, Dizdar N, Constantinescu R, Holmberg B, Jansson R, Aquilonius SM, Askmark H. Duodenal levodopa infusion monotherapy vs oral polypharmacy in advanced Parkinson´s disease. Neurology. 2005;64:216-23. • Evidence Level: Ib
