Download
1 / 8
80 likes | 400 Vues
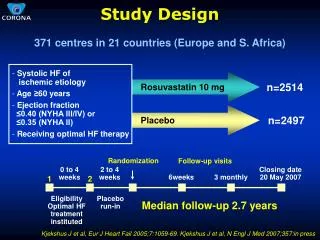
Study Design. 1 21 Relapsing-remitting MS patients randomized to Stress Management Therapy MS active treatment* 16 individual sessions conducted over 24 weeks Additional 24 weeks of follow-up Wait-list control* MS treatment as usual for 10+ months 5-hour workshop after 10th month

E N D
Study Design • 121 Relapsing-remitting MS patients randomized to • Stress Management Therapy MS active treatment* • 16 individual sessions conducted over24 weeks • Additional 24 weeks of follow-up • Wait-list control* • MS treatment as usual for 10+ months • 5-hour workshop after 10th month • MRIs performed at weeks 8,16,24,32,40, & 48 *All patients continued their usual disease-modifying therapy. Mohr DC, et al. Neurology. 2012;79:412-419.
Study Design • Primary endpoint • Cumulative number of new Gd+ lesions at weeks 8, 16, and 24 • Secondary endpoints • Cumulative number of new/enlarging T2 lesions • Patients free of new Gd+ and new T2 lesions • T2 volume change • Brain volume change • Stress • Clinical exacerbation Mohr DC, et al. Neurology.2012;79:412-419.
Reduction in Cumulative Gd+ Lesions and New T2 Lesions (24 Weeks) SMT-MS Group Control Group (n = 61) (n = 60) P Value Cumulative Gd+ lesions Number 50th percentile 0 0 75th percentile 0 1 .04 Patients free from Gd+ lesions 76.8% 54.7% .02 Absolute risk reduction: 22.2% New T2 lesions Number 50th percentile 0 1 75th percentile 1 3 .005 Patients free from new lesions 69.5% 42.7% .006 Absolute risk reduction: 26.8% Abbreviation: SMT-MS, stress management therapy – multiple sclerosis.Mohr DC, et al. Neurology. 2012;79:412-419.
Changes in Brain Volume*and Stress† SMT-MS Group Control Group (n = 61) (n = 60) P Value Brain volume % change -0.11 -0.43 .01 Stress Life Events Scale Baseline 3.1 ± 2.3 2.9 ± 2.3 Week 24 1.5 ± 1.2 1.8 ± 1.2 .04 Brief Inventory of Perceived Stress Baseline 18.2 ± 5.7 17.3 ± 6.3 Week 24 16.3 ± 6.2 17.5 ± 6.2 .007 *Assessed at 48 weeks; †Assessed at 24 weeks. Mohr DC, et al. Neurology. 2012;79:412-419.
Clinical Outcomes • No significant differences between groups in confirmed exacerbations • Baseline to week 24 • 22 in Stress Management Therapy-MS (SMT-MS) group vs 22 in control group (P = .84) • Week 24−48 • 15 in SMT-MS group vs 18 in control group (P = .40) • No significant differences between groups in Expanded Disability Status Scale over the trial period (P = .15) Mohr DC, et al. Neurology. 2012;79:412-419.
Follow-Up at 48 Weeks No statistically significant differences remained between groups in terms of • Cumulative number of Gd+ lesions • Cumulative number of new or enlarging T2 lesions • Patients remaining free of Gd+ lesions • Patients remaining free of new T2 lesions • Levels of stress Mohr DC, et al. Neurology. 2012;79:412-419.
Possible Reasons Why Benefits Were Not Maintained • Patients were able to employ the new coping skills as long as they were receiving treatment, but were unable to continue these behavioral changes without ongoing program support • Expectations on the part of patients and/or the supportive relationship provided by treatment may have accounted for the benefits of the SMT-MS intervention Mohr DC, et al. Neurology. 2012;79:412-419.
Conclusions • Stress management therapy: Effective in reducing new Gd+ lesions and new/enlarging T2 lesions, even in patients with higher disease activity • Findings provide firm evidence of the link between stress and increased MRI activity • Ongoing stress management therapy may be necessary to sustain the benefit of treatment