Download
1 / 28
280 likes | 655 Vues
Acute Pericarditis/ ECG conference. Jimmy Klemis, MD Jan 8, 2002. Pericardium. Visceral / serous Direct contact with epicardium (ST elev) single layer mesothelial cells Parietal / fibrous mesothelial and fibrous layer. Pericardial Anatomy. Visceral – transparent

E N D
Acute Pericarditis/ECG conference Jimmy Klemis, MD Jan 8, 2002
Pericardium • Visceral / serous • Direct contact with epicardium (ST elev) • single layer mesothelial cells • Parietal / fibrous • mesothelial and fibrous layer
Pericardial Anatomy Visceral – transparent Parietal – translucent Transverse sinus – curved probe
Etiology – Acute Pericarditis • Infectious • Viral : Coxsackie, Echo, EBV, Influenza, HIV • Bacterial: TB, staph, hemophillus, pneumococcal, salmonella • Fungal/other: histo/blasto/coccidio, rickettsia • Rheumatologic • SLE, Sarcoid, RA, Dermatomyositis, Ankylosing Spondylitis, Scleroderma, PAN • Neoplastic • Primary: angiosarcoma, mesothelioma • Metastatic: breast, lung, lymphoma, melanoma, leukemia • Immunologic • Celiac sprue, Inflammatory Bowel Disease • Drug • Hydralizine, Procainamide • Other • MI, Dressler’s, Post Pericardiotomy, Chest Trauma, Aortic dissection • Uremic, Post Radiation • IDIOPATHIC
Acute Pericarditis – Clinical • History • preceding viral illness, etc • Symptoms • Chest pain • Signs • Friction Rub • ECG • early: PR / ST changes • late: isoelectric ST/ T inv
History • Often preceding viral illness 1-2wk prior • Chest Pain • Sudden, sharp,pleuritic, constant • worse supine/ L lat decub, relief sitting up • radiation: back, trapezius ridge • symptoms usually resolve by 2 weeks, ECG abnormalities may persist for months
Auscultory – Rub(s) • Endopericardial (classic) • “triphasic”: atrial sys, ventricular sys, early diastole • may only hear 2 phase (afib or tachycardia) or 1 • loudest LSB, raised extremities/increased venous return • Pleuropericardial • “exopericardial”, extension into adjacent structures • marked resp variation, musical quality • Conus • dilation of pulm conus in hyperactive heart • PE, thyroid storm, acute beriberi • Pneumohydropericardium • air/gas overlying pcard fluid • metallic tinkle (small amt) ; churning/splashing “mill-wheel sound” (lg)
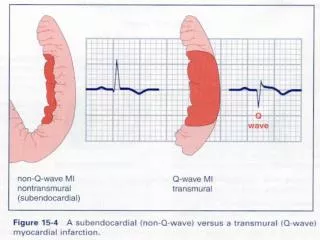
ECG • PR depression • ST elevation • concave up, ST/T V6 >.25, no reciprocal • DDx: • Acute MI • Early Repolarization • Myocarditis • Aneurysm • other: Brugada, BBB
Acute Pericarditis - Stages • Stage I • first few days 2 weeks • ST elev, PR depression • up to 50% of pt with sxs/rub do NOT have/evolve stage I1 • Stage II • last days weeks • ST returns to baseline, flat T • Stage III • after 2-3 weeks, lasts several weeks • T wave inversion • Stage IV • lasts up to several months • gradual resolution of T wave changes 1 Spodick DH, Pericardial Disease. Braunwauld 6th
Acute PCARD – Stage I, II 60 y/o man with acute PCARD on presentation and after 1 mo resolution of sxs, * Marriott’s Practical ECG 10th ed, p 208
Acute PCARD – Stage III 19 y/o Female after 1 wk in hospital with Acute Pericarditis
Cardiac Isoenzymes - ? helpful • 2 year study, ER based1 • 14 pt with 2/3 findings (CP typical for PCARD, rub, and ECG changes c/w PCARD) • 71% had elevated TropI (pk 21) with negative CAD workup • Not reliable to differentiate MI vs PCARD 1Brandt RR, et al. Am J Card 2001, June 1
Treatment • NSAIDS/ASA • ASA 650 q3-4hr • Ibuprofen 300-600 q 6-8 hrs x 1-4days • Avoid Indocin, reduces CBF • Steroids • if no response after 48hr NSAID • use concurrent NSAID • Colchicine • .6 q12 chronic +/- NSAID • useful in recurrent pericarditis • symptom free period 3.1 +/- 3mos vs 43 +/- 35mos (p<.00001) in largest multicenter trial to date1 • Anecdotal evidence of benefit in Acute PCARD, effusion 1Adler Y, et al. Circulation, 1998 June 2
Complications • Pericardial Effusion/Tamponade • Constrictive Pericarditis • can be “transient” – 10% may have transient sxs within 1st month, resolves by 3 months • Recurrent Pericarditis (20-25%) • Rx – NSAIDS/Colchicine +/- steroids
Gross Pathology “Bread & Butter” appearance Fibrinous stranding
ECG Quiz Acute Pericarditis, Stage I
ECG quiz 2 Acute Ant MI
ECG quiz 3 Early Repolarization
ECG quiz 4 Early Repolarization
ECG Quiz 5 Pericardial dz, diffuse ST elev
ECG Quiz 6a Acute antseptal MI
ECG Quiz 7 Early Repolarization
ECG quiz 8 Incomplete RBBB