Download

1 / 13
140 likes | 699 Vues
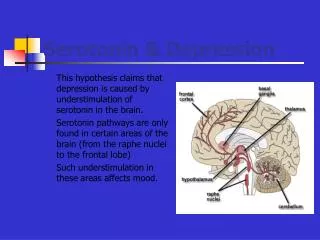
Sternbach Criteria for Serotonin Syndrome Recent addition or increase in a known serotonergic agent Absence of other possible etiologies (eg, infection, substance abuse, withdrawal, etc) No recent addition or increase of a neuroleptic agent

E N D
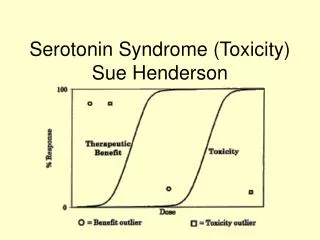
Sternbach Criteria for Serotonin Syndrome Recent addition or increase in a known serotonergic agent Absence of other possible etiologies (eg, infection, substance abuse, withdrawal, etc) No recent addition or increase of a neuroleptic agent At least 3 of the following symptoms: Mental status changes (confusion, hypomania), agitation, myoclonus, hyperreflexia, diaphoresis, shivering, tremor, diarrhea, incoordination, or fever 29 cases reported to the FDA between 1998 and 2002 of possible serotonin syndrome in patients taking triptan combined with SSRI or SNRI reading to FDA warning. Serotonin syndrome
Shapiro and Tepper (2007)-extrapolating from numbers recorded by a pharmacy benefit management company determined one million patient month exposures of triptan SSRI combination. Assuming 10 times as many cases as reported annual incidence of serotonin syndrome is less than .03%. No published reports in patients taking triptan is alone. Postmarketing study or subcutaneous triptan included 1784 patients on SSRI with no adverse events. Shapiro R , Tepper SJ; The Serotonin Syndrome, Triptans, and the Potential for Drug–Drug Interactions. HEADACHE 47; 266–269. • Serotonin syndrome mediated at 5HT 2A receptor yet triptan is agonist at 5HT1B 5HT1D. Gillman PK. Triptans, serotonin agonists, and serotonin syndrome (serotonin toxicity): A review. Headache. 2010;50:264-272. • 2007-08 1.3 million prescriptions triptan and SSRI/SNRI-90%increase from 2004-05.Of patients taking triptans 21 % are also taking SSRIs.The number of GPs prescribing has halved yet number of neurologisyts prescribing has doubled. Sclar D et al. Concomitant Use of Triptan, and SSRI or SNRI After the US Food and Drug Administration Alert on Serotonin Syndrome.HEADACHE: 52: 198–203
Mixing Triptans • 156 members of the AHS responded to a survey on prescribing habits.Of the respondents 2/3 sometoimes combine injectable sumatriptan with oral sumatriptan . 30% sometimes advise patients to combine a different triptan with injectable sumatriptan and 21% do so routinely.
Rothrock J. et al. Mixing Triptans. Headache 2011; 51: 135-140 • Patients were prescribed an oral triptan other than sumatriptan (zolmitriptan, rizatriptan, almotriptan, eletriptan,) and asked to take sumatriptan 6 mg injection for rescue medication if needed. • 200 subjects participated in the study and 184 completed. • 89% (164) of completers combined the two drugs at least once to treat a total of 903 attacks. 72% treated more than three attacks. • Of the 132 subjects who used a combination on three occasions 89% were either satisfied or very satisfied, 10% were either dissatisfied or very dissatisfied • No serious adverse events. Further study is needed
SNOOP4 • Systemic eg.fever ,wt loss-tumours,meningitis,abscess • Neurologic e.g.neurologic deficit,fits • Onset after 50 • Onset sudden Vascular events e.g. subarachnoid, cerebral vasoconstriction • Progressive • Precipitated by Valsalva e.g. Chiari malformation • Postural aggravation e.g. Low pressure headache • Papilloedema
Topiramate versus Valproate • A study comparing TPM with DVP in the real world • Patients selected had less than 15 headache days a month and were not on a prophylactic. Topiramate was titrated up to 75mg b.d. as tolerated. Valproate was titrated up to 500 b.d. as tolerated. Krymchantowski A et al.Topiramate vs Divalproex Sodium in the Preventive Treatment of Migraine: A Prospective “Real-World” Study. HEADACHE. 51; 554–558,
Results • TPM- 40/69 (58%) of patients had greater than 50% reduction. 10 were lost to follow-up, 10 patients failed to achieve 50% reduction, 6 stopped because of side-effects and 3 withdrew. • DVP-26/51(51%) of patients had greater than 50% reduction.8 were lost to follow-up, 3 failed to achieve a 50% reduction and 10 stopped due to side-effects and 4 withdrew. • From this group with a 50% reduction in headache: For TPM 17/40(42.5%) had a greater than 75% reduction in headache. For DVP 8/26 (30.7%) had greater than 75% reduction in headache • For the completers side-effects as follows: TPM-weight loss 50%, paraesthesiae 48%, cognitive disturbance 20%. DVP-weight gain 24%, hair loss 24%, 24%GI upset
Combining Topiramate and Valproate • TPM increased to 50 mg bd stages. Valproate SR increased to 1 g nocte in stages. • Patients in either group who achieved greater than 50% reduction in headache but intolerable side-effects had the dose of TPM reduced to25/50 and valproate added at a dose of500 nocte. The valproate group were reduced to 500 nocte and TPM added at 25/50. • TPM.157 pts.126 fu, 59 had 50% reduction but 22 had side effects • Valproate 102 pts, fu 78, 27 had 50% reduction but 16 had side effects.
38 patients went to next phase • TPM 17/22 (77.3%) reported a decrease in side-effects but persistence of improvement .Valproate 10/16(62.5 %) reported a decrease in side-effects but persistence of improvement .
New Daily Persistent Headache • 1. Gender: female predominance (gender ratio range 1.4-2.5:1) • 2. Age of onset: younger in women, many 2nd-3rd decade • 3. Location: bilateral in most • 4. Intensity: moderate to severe in most patients • 5. Pain duration: constant without pain free time • 6. Associated symptoms: migrainous features are common in almost all studies • 7. Recognized triggering event in <50%
New Daily Persistent Headache • Possible aetiology-Post infectious, post surgery, post toxic exposure, neck hypermobility • Doxycycline effective in 4 cases of refractory headache(tnf alpha inhibitor). Also steroids used • Rozen T. New Daily Persistent Headache: Clinical Perspective. Headache:51, 641–649, April 2011