Download
1 / 36
360 likes | 708 Vues
Theory of HFV. Gas Transport Mechanisms Oxygenation Ventilation. HFV Gas Exchange. Henderson first published his findings in 1915, assessing dead space relationship in ventilation.

E N D
Theory of HFV • Gas Transport Mechanisms • Oxygenation • Ventilation
HFV Gas Exchange • Henderson first published his findings in 1915, assessing dead space relationship in ventilation. • He stated, “there may easily be a gaseous exchange sufficient to support life even when VT is considerably less than dead space.”
HFV Gas Exchange • Chang theorized that convective processes were more predominant with an increase in VT and lower frequencies. A diffusive mechanism may be more predominant where there is a decrease in VT and higher frequencies are used.
HFV Gas Exchange • In the 1970’s, Bunnell and his associates demonstrated in animals that adequate alveolar ventilation could be achieved with a frequency between 5 - 30 Hz and a VT of 20 - 25% less volume than anatomical dead space. • Slutsky, et al. theorized that the gas exchange mechanism was caused by the “coupled effects” of convection and molecular diffusion.
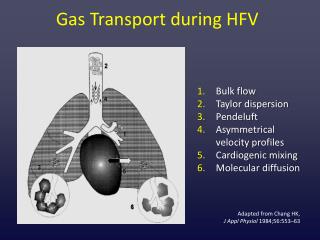
Theory of HFV Gas Exchange • Gas exchange is enhanced by additive mechanisms to the bulk flow and molecular diffusion of conventional ventilation. • 6 mechanisms for gas exchange have been noted with high frequency ventilation
How does HFV work? • Convection (Bulk Flow) Ventilation • Even with small tidal volumes, direct alveolar ventilation occurs to short path length units that branch off of the primary airways.
How Does HFV Work? • Taylor Dispersion: • Convective flow superimposed on a diffusive process, results in increased dispersion of the tracer molecules. • The high velocity spike of gas moves down the center of the tube, leaving the molecules on the periphery unmoved. Gas diffuses evenly through the tube when flow stops.
How Does HFV Work? • Asymmetrical Velocity Profile • During inspiration, the high frequency pulse creates a “bullet” shaped profile, with the central molecules moving further down the airway than those molecules found on the periphery of the airway. • 2 “ Steps Forward”
How Does HFV Work • Asymmetrical Velocity Profile • On exhalation, the velocity profile is blunted so that at the completion of each return, the central molecules remain further down the airway and the peripheral molecules move towards the mouth of the airway. • 1” Step Back”
How Does HFV Work? • Pendeluft: • At high frequencies, distribution becomes strongly influenced by time constant inequalities. Gas from fast units (short time constants) will empty into the slow (long time constants) units.
How Does HFV Work? • Cardiogenic Mixing: • The heart beat adds to the the peripheral gas mixing.
How Does HFV Work? • Molecular Diffusion: • Is felt to be one of the major mechanisms for gas exchange in the alveolar regions. • It is responsible for the gas exchange across the AC membrane and also contributes to the transport of O2 and CO2 in the gas phase near the membrane. • This may be due to the increased turbulence of molecules.
Theory Of Operation Oxygenation and CO2 elimination have been demonstrated to be decoupled with HFOV.
Oxygenation • Oxygenation is primarily controlled by the Mean Airway Pressure (Paw) and the FiO2 for “Diffuse Alveolar Disease” (DAD). • Ventilation is primarily determined by the stroke volume (Delta-P) or the frequency of the ventilator.
Oxygenation • The Paw is used to inflate the lung and optimize the alveolar surface area for gas exchange. • Paw = Lung Volume
Oxygenation • The Paw is used to inflate the lung and optimize the alveolar surface area for gas exchange. • Paw = Lung Volume
Oxygenation • Paw is created by a continuous bias flow of gas past the resistance (inflation) of the balloon on the mean airway pressure control valve.
Oxygenation • The Paw of the oscillator without the piston moving is a “TRUE CPAP” system. • The Paw is changed by adjusting the bias flow or the inflation of the balloon control valve (Paw Adjust).
Oxygenation • CLINICAL TIPS- • Must have adequate MAP and hemodynamic performance. Perfusion must be matched to ventilation for adequate oxygenation. • Chest x-rays and oximetry are necessary.
Oxygenation • CLINICAL TIPS- • PVR is increased with either atelectasis (Loss of support for extra-alveolar vessels) or over expansion (Compression of alveolar capillary bed). The lung must be recruited, but guard against over expanding. • Utilize x-rays and oximetry to wean Paw when rapid improvement in compliance yields lung overexpansion.
Oxygenation • For a DAD process, increase the Paw to achieve adequate arterial oxygenation (88 - 93% SaO2). • Increase the Paw in 1 - 2 cm increments every 5 - 10 minutes to achieve adequate oxygenation as reflected by the oximeter.
Oxygenation • In ALS, use a lower Paw and Delta-P to minimize further injury and allow the leak to seal • Low Lung Volume Strategy with Right Posterior Hemi-diaphragm at 7 - 8 rib level expansion for neonates. • Use higher FiO2’s and less than optimal ABG’s: PaO2 in the 50’s with acceptable hypercarbia and pH > 7.25
Oxygenation • Maintain the Paw and decrease the FiO2 until it is at 60% or lower. • Re-check a CXR for lung volume • If the diaphragm is between 8 and 8-1/2, continue decreasing the FiO2. • If the diaphragm is between 9 and 9-1/2, decrease the Paw 0.5 to 1 cmH2O • Continue weaning FiO2
Ventilation • Controlled by the movement of the pump/piston mechanism. • Alveolar Ventilation during CMV is defined as: f x Vt • Alveolar Ventilation during HFV is defined as: f x Vt 2 • Therefore, changes in volume delivery (as a function of Delta-P, Frequency, or % Insp. Time) has the most significant affect on CO2 elimination.
Ventilation • Primary control of CO2 is by the stroke volume produced by the Power Setting • The amplitude or Delta-P measurement displayed on the front panel is produced by adjustment of the Power Setting
Ventilation • The amplitude is created by the distance that the piston moves, resulting in a volume displacement and a visual CHEST Wiggle. • It may also be described as the peak-to-trough swing across the mean airway pressure.
Ventilation • Secondary control of PaCO2 is the Frequency set. • If the Power controls the force with which the piston moves, the Frequency controls the time allowed (distance) for the piston to move. • Therefore, the lower the frequency setting, the greater the volume displacement, and the higher the frequency setting, the smaller the volume displacement.
Ventilation • Recommended Guidelines for initial Frequency Setting: (May be disease dependent) • < 2000 gms 15 Hz • 2 - 12 kg 10 Hz • 13 - 20 kg 8 Hz • 21 - 30 kg 7 Hz • > 30 kg 6 Hz
Frequency • Frequency MAY or MAY NOT have to be adjusted from the initial setting • Frequency is not weaned as is done with CMV (decreasing frequency with HFOV increases ventilatory support).
Ventilation • The % Inspiratory Time also controls the time for movement of the piston, and therefore assists with CO2 elimination. • Do Not manipulate the % I-Time for frequencies of 10 - 15 Hz. This may potentially increase inadvertent gas trapping. • Increasing % I-Time is used in larger pediatric patients as the third maneuver to control CO2 elimination.
Ventilation • The ET tube acts as a filter to the pressure wave, attenuating the pressure as great as 90% with a 2.5 ET tube. The larger the tube the less attenuation. • The amplitude shown on the LED read out is measured within the circuit • HFOV is considered a VERY GENTLE form of ventilation.
Ventilation • Distal amplitude measurements with alveolar capsules in animals, demonstrate it to be greatly reduced or “attenuated” as the pressure traverses through the airways. • Due to the attenuation of the pressure wave, by the time it reaches the alveolar region, it is reduced down to .1 - 5 cmH2O.
Ventilation • Bias Flow produces the Paw of the system, and also helps to flush the CO2 that is actively pulled back into the circuit during the expiratory phase. • If decreasing the PaCO2 is difficult, increasing the bias flow through the system may be helpful.
Clinical Tips • If increasing the amplitude has no net affect on decreasing the PaCO2, consider decreasing the Frequency setting by 1 Hz at a time. • If there is minimal CWF, and the PaCO2’s are too low, consider increasing the Frequency setting by 1 Hz. • With cuffed ET tubes, minimally deflating the cuff may allow airway wall CO2 to exit the circuit at the tip of the tube.
THEREFORE • If the Paw = CPAP • And the Amplitude = Chest Wiggle • Then HFOV can be defined as • CPAP with a Wiggle! • Not nearly as complicated a concept as some try to make it!
SUGGESTED READING • Chang HK. Mechanisms of gas transport during ventilation by HFOV, Brief Review, J Appl Physiol, 1994 • Schindler M, et al. Effect of Lung Mechanics on Gas Transport During HFO. Pediatric Pulmonology, 1991 • SensorMedics Critical Care, Operator’s Manual for the 3100A, 1995