Download
1 / 36
360 likes | 489 Vues
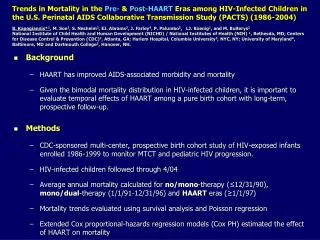
Morbidity and Mortality in the HAART era. Andrew Phillips Royal Free & University College Medical School London. Death in the HAART era: rates and reasons. Trends in death rate: HOPS. Trends in death rate over calendar time in UK. Rate per 100 people. Number of deaths in year

E N D
Morbidity and Mortality in the HAART era • Andrew Phillips • Royal Free & University College Medical School • London
Death in the HAART era: rates and reasons
Trends in death rate over calendar time in UK Rate per 100 people Number of deaths in year Number seen for care in year 96 97 98 99 00 01 02 03 04 05 06 Year Deaths 1481 749 514 472 484 477 520 572 495 539 497 15 16 18 20 22 26 32 36 41 46 52 Seen for care(thousands,rounded) Source: HPA
Breakdown of causes of death: France 2005 AIDS Cancer Hepatitis C CVD Suicide Non-AIDS infection Accident Hepatitis B Liver disease OD / drug abuse neurologic renal pulmonary digestive iatrogenic metabolic psychiatric other unknown N = 937 deaths ANRS EN19 Mortalité 2005 Lewden et al, CROI 2007 Percent
Audit of 397 deaths in UK 2005: Scenario leading to AIDS-related deaths Scenario % of AIDS deaths Diagnosed too late for effective treatment 40% Under care, but with untreatable complication 29% Treatment ineffective due to poor adherence 12% Chose not to receive treatment 8% Known HIV, not under regular care, 6% re-presented too late MDR HIV, ran out of options 5% BHIVA Audit – Johnson et al 2006
Incidence of non-AIDS death 1994-2004 (excluding death from unknown causes) Rate per 100 person years Test for trend: p < 0.0001 95 96 97 98 99 00 01 02 03 04 Year EuroSIDA; Mocroft, Lundgren et al, personal communication
Might HIV increase the risk of serious non-AIDS conditions and non-AIDS death ?
Might HIV increase the risk of serious non- AIDS conditions and non-AIDS death ? • Incidence of, and death from: • - Non-AIDS malignancies • - End stage renal disease • - Cardiovascular events • - Liver cirrhosis • - Deaths from other non-AIDS causes • Not focussing on adverse effects of ART
Possible mechanisms: General • - Very early loss of CD4 T cells in gastrointestinal tract • Loss of immunological and epithelial integrity of the mucosal • barrier – leading to microbial translocation • Generalized immune activation • - Fibrosis of lymphatic tissue Veazey et al, Science 1998 Brenchley et al, Nature Med 2006 Brenchley, J Exp Med 2004 Schacker et al, Clin Vacc Immunol 2006
Possible mechanisms: Non-AIDS malignancies • Immunodeficiency, leading to: • - reduced control of oncogenic pathogens • - damage due to infections and resulting • chronic inflammation • - loss of ability to identify transformed cells Littman et al. Cancer Epidemiol Biomarkers Prev 2005
Possible mechanisms: Kidney disease • HIV associated nephropathy (HIVAN) • (viral nephritis reversed by ART) • Link with other kidney pathologies (e.g. • immune complex glomerulonephritis) • High prevalence of proteinuria, associated • with HIV RNA level and CD4 count • HIV RNA and CD4 count predict raised • creatinine levels • proteinurea & elevated creatinine associated • with all cause mortality in HIV patients Szczech et al, Kidney International 2002 Lucas et al, AIDS 2004 Szczech et al, Kidney International 2004 Kimmel et al, Ann Intern Med 2003
Possible mechanisms: Cardiovascular disease • Association of HIV-infection with adverse • changes in known or potential biomarkers for • CVD. • HDL-cholesterol depletion • Inflammation (raised IL-6, C-reactive protein) • Endothelial activation/dysfunction (VCAM, ICAM) • Activation of coagulation (D-dimer) • Several of the changes appear to be at least • partially reversed by ART Riddler JAMA 2003 de Larranaga et al, Blood Coag. & Fibrinolys 2003 Lau et al, Arch Intern Med 2006 Wolf et al, J Infect Dis 2002
Possible mechanisms: Liver disease • immunodeficiency linked to more • rapid progression of liver fibrosis in • HBV and HCV infected people • affect CD4+ and CD8+ response to • HBV / HCV • - alter HBV / HCV quasi-species • increased hepatocyte apoptosis Tan et al, Current HIV research 2006 Thio et al, Lancet 2002 Eyster et al, JAIDS 1993 Soto et al, J Hepatol 1997
Might HIV increase the risk of serious non- AIDS conditions and non-AIDS death ? Types of evidence comparison of risk of serious non-AIDS events between HIV-infected and HIV-uninfected people studies of the association between CD4 count (and HIV RNA) and risk of serious non-AIDS events randomized trials of the impact on serious non- AIDS events of reduction in HIV RNA level and increase in CD4 count with ART
Comparison of risk of events between HIV- infected and HIV-uninfected people: limitations • HIV -ve comparison group will differ from HIV-infected • group in more ways than just the HIV infection (eg smoking) • Adjustment for such confounding bias may not be possible. • Each non-AIDS condition has its own set of risk factors • which could act differently in HIV-infected people. • HIV infected subjects often mixture of those on ART and • ART-naïve, so not possible in all studies to distinguish • effect of HIV from effect of ART.
HIV and risk of non-AIDS malignancies Meta-analysis: 444,172 people with HIV, 31,977 transplant patients For 20 / 28 cancers examined there was significantly increased incidence in both groups – strongly suggesting a link with immunodeficiency Standardized Incidence Ratio HIV/AIDS Transplant Lung 2.7 2.2 Leukaemia 3.2 2.4 Kidney 1.5 6.8 Oesophagus 1.6 3.1 Stomach 1.9 2.0 Grulich et al, Lancet 2007
HIV and risk of lung cancer, independent of smoking CID 2007 AIDS 2007
HIV and risk of End Stage Renal disease U.S. Veterans without diabetes Hazard ratio for End Stage Renal Disease # people # ESRD Hazard ratio* White HIV -ve 1,201,870 3991 1.0 HIV +ve 6,139 13 0.8 (0.5 – 1.3) Black HIV -ve 206,636 1425 2.0 (1.9 – 2.2) HIV +ve 6,816 129 4.6 (3.4 – 6.1) *Adjusted for age, sex, baseline eGFR category, CAD, HTN, heart failure, COPD, PVD, HCV infection, cerebrovascular disease, and SES. Little effect of HIV in diabetics Choi et al J Am Soc Nephr 2007
HIV and Cardiovascular Disease Subject source N CVD Risk in HIV + cases in vs. HIV –ve HIV + Klein Administrative & 72 Increased clinical management database Mary-Krause HIV cohort / 60 Increased in those general population with > 18 m PI use Currier Adminstrative 1360 Increased at database younger ages Triant Patient Data 189 Increased Registry Klein et al, JAIDS 2002 Mary-Krause et al, AIDS 2003 Currier et al, JAIDS 2003 Triant et al, J Clin Endocrin Metab 2007
HIV and Liver disease 4865 men and boys with haemophilia (and probable HCV infection), of whom 1218 HIV-infected HIV (and haemophilia) status 25 year cumulative risk of liver death Severe haemophilia, not HIV 1.4 (0.7 – 3.0) Moderate / mild haemophilia, not HIV 1.2 (0.5 – 2.6) HIV-infected (all haemophilia severities) 6.5 (4.5 – 9.5) Darby et al, Lancet 1997 Similarly for HBV in MACS– Thio et al, Lancet 2002
All cause death rates in ART-naïve patients with CD4 count > 350 /mm3, compared with the general population Abstract N-264 Wednesday 10.30 - Lodwick et al
Might HIV increase the risk of serious non- AIDS conditions and non-AIDS death ? Types of evidence comparison of risk of serious non-AIDS events between HIV-infected and HIV-uninfected people studies of the association between CD4 count (and HIV RNA) and risk of serious non-AIDS events randomized trials of the impact on serious non- AIDS events of reduction in HIV RNA level and increase in CD4 count with ART
CD4 count and risk of death: DAD and CASCADE 1.6 1.2 CASCADE (ART-naïve) 0.8 Rate / 100 person years 95% CI 0.4 0.0 Non-AIDS causes All causes 1.6 1.2 DAD 0.8 0.4 0.0 200 – 350 – > 500 349 499 200 – 350 – > 500 349 499 Weber at al Marin et al CD4 count (/mm3)
Hospitalization events according to cause and CD4 count: Aquitaine cohort, 2000-2004 3863 patients Number of hospitalizations Number (mean per patient) during 2000-2004 CD4 count of patients > 500 2442 16 (0.01) 335 (0.14) 351 (0.14) 200-499 2922 60 (0.02) 581 (0.20) 641 (0.22) < 200 1229 260 (0.21) 439 (0.36) 699 (0.57) AIDS non-AIDS All p < 0.001 p < 0.001 ANRS C03 Aquitaine Cohort Bonnet et al, HIV Medicine 2007
HIV RNA and risk of serious non-AIDS events: SMART All serious non-AIDS Non-AIDS malignancy Renal CVD Liver Other non-AIDS death 0.2 0.5 1.0 1.5 Adjusted hazard ratio < 400 vs. > 400 copies/mL Adjusted for age, gender, prior AIDS, hep B/C, smoking, latest CD4 count SMART, unpublished
Might HIV increase the risk of serious non- AIDS conditions and non-AIDS death ? Types of evidence comparison of risk of serious non-AIDS events between HIV-infected and HIV-uninfected people studies of the association between CD4 count (and HIV RNA) and risk of serious non-AIDS events randomized trials of the impact on serious non- AIDS events of reduction in HIV RNA level and increase in CD4 count with ART
SMART Study Participants with CD4 count > 350 84% on ART, 16% off ART Randomization n = 2752 n = 2720 Intermittent ART Stop or defer ART when CD4 count > 350, restart or start ART when CD4 count < 250 Continuous ART Follow-up 33% on ART 96% CD4 > 200 94% on ART 99% CD4 > 200 N Engl J Med 2006
Risk of serious non-AIDS events in SMART Number of events Intermittent Continuous ART ART 113 73 All serious non-AIDS Non-AIDS malignancy 27 24 Renal 9 2 CVD 48 31 Liver 10 7 Other non-AIDS death 30 16 0.5 1 2 3 5 10 Of the 85 deaths that occurred in SMART, only 7 (8%) were from AIDS diseases Hazard ratio Intermittent ART vs. Continuous ART SMART Study Group, NEJM 2006 &Neaton et al, Current Opinion in HIV/AIDS 2008
Risk of serious non-AIDS events in SMART: patients ART naïve or off ART for > 6 months N = 477 patients Number of events Hazard ratio Deferred vs. Deferred Immediate Immediate ART ART ART (95% CI) p-value 12 2 7.02 (1.57 – 31.4) 0.01 Emery et al, JID (in press)
Inflammatory and coagulation markers in SMART • Abstract D-60 Wednesday 10.00 – Kuller et al • Illustrates value of biomarker studies based on stored • samples from a randomized trial with clinical endpoints
Might HIV increase the risk of serious non-AIDS conditions and non-AIDS death ? • Summary • On balance, evidence suggests HIV may well play a role in • several serious non-AIDS defining events. • In the upper CD4 count range, while overall risk of any disease is • relatively low, non-AIDS events are much more common than • AIDS events. • Given the associations with latest level of CD4 count / HIV RNA • and the results from SMART use of ART may well reduce risk of • some serious non-AIDS events.
What steps can we take towards further reduction in morbidity and mortality ?
What steps can we take towards further reduction in morbidity and mortality ? • Continued efforts to diagnose HIV as early as possible • Research into prediction of non-AIDS events in context of HIV • - ART-naïve and ART-treated • - standardize diagnostic criteria and data collection methods • Trial of ART initiation in people with CD4 count > 500 /mm3 • - non-AIDS diseases relatively common at higher CD4 count • - SMART suggests risk / benefits of ART favour benefit • - durable virological benefit of current ART • - cost-effectiveness / reduction in transmission risk • - basis for identifying biomarkers that mediate raised • risk, providing insights into mechanisms (also beyond HIV)
Conclusions • The study of serious non-AIDS conditions is an important • emerging area for HIV research • Research is needed to provide a basis for defining models • of care for people with HIV which take into account the risk • of all serious conditions • Research into mechanisms by which HIV affects risk of non- • AIDS conditions is needed, and it may help us understand • more about the causes of such conditions outside HIV • - The possibility that ART should be initiated much earlier • should be investigated in a randomized trial. Such a trial • will form a key resource for this new research area.
Acknowledgements Jens Lundgren, Jim Neaton HIV Epidemiology & Biostatistics Group, Royal Free, UCL Caroline Sabin, Amanda Mocroft, Fiona Lampe, Alessandro Cozz-Lepri, Colette Smith, Zoe Fox, Wendy Bannister, Loveleen Bansi, Rebecca Lodwick, Joanne Reekie DAD (Aquitaine, Nice, CPCRA, EuroSIDA, ICONA,SHCS, Brussels, BASS, AHOD, ATHENA, HivBivus) EuroSIDA SMART FIRST CASCADE HOPS Extra analyses: Jacquie Neuhaus (SMART), Grace Peng, Jason Baker (FIRST), Benoit Marin, Genevieve Chene, Abdel Babiker (CASCADE), Colette Smith, Caroline Sabin (DAD), Amanda Mocroft (EuroSIDA)