Download
1 / 33
330 likes | 452 Vues
Disease and Demography in British India: The Influenza Pandemic of 1918-19. Siddharth Chandra, Eva Kassens-Noor , Goran Kuljanin , Joshua Vertalka , Jennifer Wray Michigan State University Presentation prepared for “A Workshop on World-Historical Dataverse Vision and Research”.

E N D
Disease and Demography in British India: The Influenza Pandemic of 1918-19 Siddharth Chandra, Eva Kassens-Noor, GoranKuljanin, Joshua Vertalka, Jennifer Wray Michigan State University Presentation prepared for “A Workshop on World-Historical Dataverse Vision and Research”
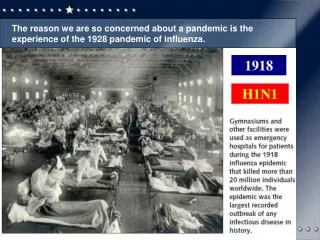
The Influenza Pandemic of 1918-19: Background • Single most deadly short-term epidemic of the 20th century • Duration – 6-9 months • Worldwide mortality (25-50 million) • Some estimates as high as 100 million • Exceeded combined death toll from World War I and World War II • Johnson and Mueller (1992) • India was the single worst hit country • “The mother of all pandemics” • Taubenberger and Morens (2006)
Prior work on the 1918-19 Influenza in India • Primary source: sanitary and public health reports of India and the provinces • Government of India, various years, for example • Usual “flu-like” symptoms • A common complication is pneumonia • Excess mortality is largest for people in the prime of life • Not infants and elderly people as is usually the case
Major research questions • How many people died in India? • Presented at World-Historical Dataverse workshop, February 2011 • Chandra, Kuljaninand Wray (2012) • How is this related to population growth before and after the pandemic? • Presented at World-Historical Dataverse workshop, February 2011 • What geographic patterns do we see? • Focus of this presentation
Geographic patterns of the pandemic • Data source • Sanitary and public health reports • Nine major provinces • 199 districts • Six “chief diseases” of India • Monthly mortality data by district • Mortality data are highly unreliable • Underreporting • Problematic categories • Diarrhea & dysentery, respiratory diseases, fevers, cholera, plague, smallpox
Obtaining Information about Influenza from Colonial Data • Most deaths from influenza reported under “fevers” category • But fever deaths include other major causes, especially malaria • Cannot be used as-is to investigate influenza mortality itself • However, the data still reveal patterns about timing • Peak monthly fever mortality over the period 1916-1920 always • occurs between September 1918 and January 1919 and • is much higher than “background” fever mortality • see over for example
Methodology • Use monthly fever mortality data for five-year period 1916-1920 • 60 monthly observations for 199 districts • Estimate weekly mortality using monthly time series • 60*52=3120 weekly observations per district • Rank weeks on the basis of fever mortality • Top four weeks vs. all other weeks
Estimated Spread of Influenza Across India www.youtube.com/watch?v=9s9LUzkFjp8 (Password protected, please refer to following slides)
Findings • Pandemic peaks between September 22, 1918 and January 19, 1919 • Rapid spread • Three sub-waves • Monthly spacing between sub-waves
Findings • First sub-wave • Entry through Bombay (west) • Madras (south) and Puri (east) • Peak: week of October 13 • Second sub-wave • Punjab (northwest), Central Province (central), sub-Gangetic region (north central) • Peak: weeks of November 10/November 17 • Third sub-wave • North of the Ganges (north) • Peak: weeks of December 6/December 15
Future Research • How rapidly did the disease spread? • What are the correlates of spread? • Enablers and inhibitors • Human and non-human • Possible adaptations of epidemiologic models for aggregate data as well • Colonial data are rich • Data inventory for project • Excel spreadsheet showing variables collected to date
Conclusions • Historical data such as those collected by the sanitary authorities in British India can provide valuable insights into important questions in public health and demography • While the raw data may not be presented in the most desirable form, they can still be leveraged for valuable insights • Modern methodologies need to be deployed to analyze these data to obtain these insights
References • Chandra, Siddharth, GoranKuljanin, and Jennifer Wray. 2012. “Mortality from the Influenza Pandemic of 1918-19: The Case of India.” Demography, in press. • Government of India. Various years. Annual Report of the Sanitary Commissioner with the Government of India. Calcutta: Superintendent, Government Printing. • Johnson, Niall P. A. S. and Juergen Mueller. 2002. “Updating the Accounts: Global Mortality of the 1918-1920 “Spanish” Influenza Pandemic.” Bulletin of the History of Medicine 76(1): 105-115. • Patterson, K. David, and Gerald Pyle. 1991. “The Geography and Mortality of the 1918 Influenza Pandemic .” Bulletin of the History of Medicine 65(1): 4-21. • Taubenberger, J.K. and D.M. Morens. 2006. “1918 Influenza: the mother of all pandemics.” Emerging Infectious Diseases 12(1): 15-22.
Acknowledgements This project was conceived as part of the World-Historical Dataverse project at the University of Pittsburgh This research was funded in part by a grant (1R21DA025917, PI: Chandra) from the National Institute on Drug Abuse (NIDA) of the National Institutes of Health. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of NIDA.