
Cardiovascular drugs -2
E N D
Presentation Transcript
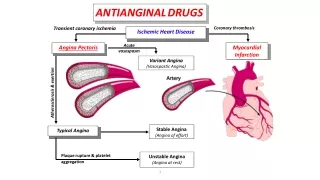
ANTIANGINALDRUGS Coronary thrombosis Transient coronary ischemia Ischemic Heart Disease Acute vasospasm Angina Pectoris Myocardial Infarction Variant Angina (Vasospastic Angina) Atherosclerosis & exertion Stable Angina (Angina of effort) Typical Angina Plaque rupture & platelet aggregation Unstable Angina (Angina at rest) 1
Goal Of Antianginal Drugs: To restore balance between Myocardial O2Demand and Supply
1. Organic Nitrates O2N O O2N NO2 O O O NO O O O NO2 O NO2 Isopentyl Nitrite, Amyl Nitrite Glyceryl Trinitrate, Nitroglycerin Isosorbid Drinitrate, Isordil The most prominent pharmacological action of organic nitrates is relaxation of vascular smooth muscles, both arterial and venous. This class of compounds has a property of generating the unstable and lipophilic free radical nitric oxide (NO) in situ PREPERATIONS: l- short acting : sublingual tablets: - gleceryl trinitrate ( nitroglycerin ) 10-30 min - isosorbide dinitrate 10-60 min also as sublingual spray
ll- long acting : nitroglycerin: - oral S.R 6-8 h - ointment 3-6 h - buccal S.R. 3- 6 h - transdermal patch 8-10 h isosorbide dinitrate: - chewable 2-3 h - oral S.R. 4-6 h isosorbide mononitrate: - oral S.R. 6-10 h erythrityl tetranitrate 6- 8 h pentaerythritol tetranitrate 6- 8 h
Structure Nitrate Esters RO H + alcohol nitrous acid alkyl nitrite water + H2O RO N O H O N O _ _ O O + + RO H + + RO N H2O H O N O O alcohol nitric acid alkyl nitrate water • Some nitrate esters are wrongly named, e.g., amylnitrite is actually isoamylnitrite, nitroglycerin is not a nitro compound Nitrate esters are susceptible to hydrolysis! Shelf life is a concern. •
2. Calcium Channel Blockers CCBs Calcium ions are known to play a critical role in many physiological functions. Inhibition of Ca+2ion influx into the myocardial cell may be advantageous in preventing angina. Vascular smooth muscles & cardiac tissue depend on calcium influx for contraction. Types of Calcium Channel Blockers • Dihydropyridines Nifedipine and others Verapamil and Bepridil • Phenylalkylamines • Benzothiazipines Diltiazem
3. b b-Blockers • Propranolol • Atenolol • Metoprolol • Nadolol 4. Other Antianginal Drugs (Coronary VDs):
3. DRUGS FOR HEART FAILURE Congestive heart failure CHF is a complex clinical syndrome characterized by impaired ventricular performance (impaired cardiac output), exercise intolerance, a high incidence of ventricular arrhythmias, and shortened life expectancy. The signs and symptoms of heart failure include tachycardia, decreased exercise tolerance and shortness of breath, peripheral and pulmonary edema, and cardiac hypertrophy. Virtually all forms of heart disease can lead to heart failure, with coronary artery disease, hypertension, and diabetes mellitus being the most common. The primary goal in treating heart failure is to improve the patient's quality of life by reliving the symptoms and to decrease the mortality rate. 15
Three categories of drugs are used in the treatment of CHF: 1. Positively Inotropic Drugs: a. Cardiac Glycosides. b. Adrenergic Receptors Agonists. c. Phosphodiestrase Inhibitors 2. Vasodilators: a. ACEIs. b. CCBs c. Organic Nitrates. 3. Diuretics (mainly potassium sparing). 17
1. Positively Inotropic Drugs (Cardiotonics) a. Cardiac Glycosides • The cardiac glycosides inhibit the Na+/K+-ATPase pump, which causes an increase in intracellular Na+, slowing the rate of the Na+/Ca++-exchanger, thereby causing an increase in intracellular Ca++leading to greater myofibebril shortening (contraction). O O OH O Digitoxose (Dig) H O OH H H OH H O O Dig3 H Digoxin, Lanoxine®
R defines the class Structure R H OH H OH O O H O O O O H O OH OH Aglycone Portion Sugar Portion • The R group at the 17-position defines the class of cardiac glycoside. Two classes have been observed in Nature: The cardenolides have an unsaturated butyrolactone ring. • The bufadienolides have an a-pyrone ring (not used therapeutically due to high toxicity). • 19
SAR of Cardiac Glycosides 1. The sugar moiety appears to be important only for the partitioning and kinetics of action. It possesses no biological activity. 2. The "backbone" U shape of the steroid nucleus appears to be very important. Structures with C/D trans fusion are inactive. 3. Conversion to A/B trans system leads to a marked drop in activity. Thus although not mandatory A/B cis fusion is important. 4. The 14 b-OH groups is now believed to be dispensible. A skeleton without 14 b-OH group but retaining the C/D-cis ring fusion was found to retain activity. 5. Lactones alone, when not attached to the steroid skeleton, are not active. Thus the activity rests in the steroid skeleton.
b- b b-Adrenergic Agonists “β-blockers” Standard therapy for treatment of CHF Cheap! Reduce sudden death caused by other drugs Propranolol: prototype Carvedilol: combination effects
c- Phosphodiesterase Inhibitors • Phosphodiesterases are responsible for the degradation of cyclic adenosine monophosphate (cAMP). increase the concentration of cAMP and the Ca2+level in the myocardial cell. Inhibition of these enzymes lead to NC H2 N O N O N N N H H Amirinone, Inocor® Milrinone, Primacor® Primarily used for management of acute heart failure Positive inotropic effects Increase rate of myocardial relaxation Decrease total peripheral resistance and afterload