Download
1 / 9
100 likes | 710 Vues
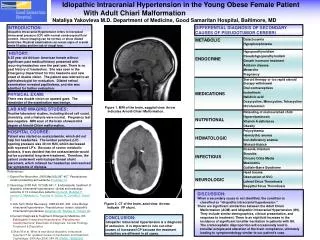
Case 65. Thyroidectomy in Patient with Hypertension. A 38 year old man is scheduled for thyroid goiter surgery. He has a history of hypertension and has been on metaproterenol and captopril. BP: 180/110, PR: 80/min ECG no specific ST-T changes. Preoperative Evaluation.

E N D
Case 65 Thyroidectomy in Patient with Hypertension A 38 year old man is scheduled for thyroid goiter surgery. He has a history of hypertension and has been on metaproterenol and captopril. BP: 180/110, PR: 80/min ECG no specific ST-T changes.
Preoperative Evaluation • History: symptoms of hyperthyroidism such as anxiety, fatigue, heat intolerance, diarrhea, dyspnea, and palpitations • PE: BP, T, HR(tachycardia?), rhythym(tachydysrhythmias?), goiter, Thyrotoxic myopathy(proximal weakness), exophthalmos • PMH: Hypertension, asthma
Preop/Labs/Tests • TSH, T3, T4 • Is patient euthyroid? • CBC, LFT, ECG • CT neck, flow-volume loops • Airway obstruction?
Preop Medication • Clonidine • Will blunt sympathetic nervous response • Midazolam • No anticholinergics • Interfere with heat regulation and contribute to increased heart rate
Induction Anesthesia/Muscle Relaxants • Thiopental • Thiourea structure with antithyroid activity • NDNM or succinyl choline
Alternate Intubation Plan • Awake intubation with fentanyl
Maintenance Anesthetic Agents • Sevoflurane/nitrous oxide mixture • Suppresses sympathetic nervous system • Possibly avoid Desflurane • Large bolus can cause transient increase in sympathetic activity • Alternate is short-acting opioid/nitrous oxide • However, does not reliably suppress sympathetic nervous system.
Intraoperative Medical Care • Thyroid storm, which mimics malignant hyperthermia, can consist of hyperthermia, tachycardia, CHF, low intravascular volume, and shock • Chilled crystalloid infusion • Continuous esmolol infusion • Propylthiouracil, methimazole, NaI • If persistent hypotension, then Dexamethasone • Inhibits T4 to T3 conversion • No aspirin • Increases level of free T4 • Elevated BP • Esmolol
Early Postoperative Care • Thyroid storm usually occurs 6-18 hrs post-op • Other Complication: • Recurrent laryngeal nerve injury • Hematoma • Tracheomalacia • Hypoparathyroidism • Superior laryngeal nerve injury • Pain management - PCA