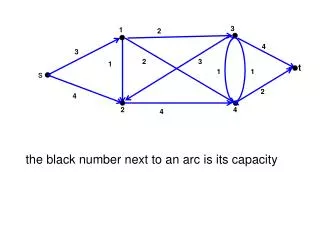
How do we describe disease-specific changes in respiratory function? 3/2 and 3/4
How do we describe disease-specific changes in respiratory function? 3/2 and 3/4. Friday Lab 7-7:50 am we can review spirometry for the lecture assignment and lab exam. How does the Bohr Effect improve oxygen delivery to a tissue that is working? What are the typical lung volumes?

How do we describe disease-specific changes in respiratory function? 3/2 and 3/4
E N D
Presentation Transcript
How do we describe disease-specific changes in respiratory function? 3/2 and 3/4 • Friday Lab 7-7:50 am we can review spirometry for the lecture assignment and lab exam. • How does the Bohr Effect improve oxygen delivery to a tissue that is working? • What are the typical lung volumes? • What are the three kinds of pneumothorax? • What are some common terms used to describe ones breathing pattern and gas imbalances? • What are the typical partial gas pressures?
A Spirometer is used to measure Breathing Patterns and Lung Volumes: Reduce these values about 20% in females. Approximate Volumes: memorize these numbers: Total Lung Capacity: TC=5-6 Liters Vital Capacity: VC=5 L…its what you can manipulate Tidal Volume: TV=500 ml Typical size of a typical resting breath • Inspiratory Reserve Volume: IRV=3L Air added to a tidal volume with Max Inspiration • Expiratory Reserve Volume: ERV=1.5L Amount you can exhale after a typical Tidal Exhalation • Residual Volume: RV=1L Air that’s left in Trachea, Bronchi, etc after a max. expiration
In our Respiratory Physiology lab we will use an electronic spirometer that converts air velocity and flow into respiratory volumes using a set of computer algorithms. Old School Spirometer
For lecture and lab tests: Calculate Breathing Rate, IRV, TV, ERV, FEV1, % FEV1 and MRV. Assume person is 140 pound 20 year old woman who is 6 feet tall, plays basketball a lot, but recently seems out of breath a lot. Are values normal or abnormal? Why?
Air Flow Distribution into tinier and tinier passages that lead to the dead-end Alveoli for gas exchange: • Entry: Oral Cavity/Nasal Cavity • Pharynx • Larynx/Glottis • Trachea • Primary Bronchi • Secondary Bronchi • Tertiary Bronchi • End cartilaginous rings • Bronchiole Above this its called Dead Space: no significant gas exchange Terminal B.Respiratory Bronchioles: some gas exchange • Alveolar Ducts-Alveoli • Most Gas Exchange is Here! (in a healthy lung)- • Describe carbon dioxide and oxygen transfer to/from blood/air
Why do we WANT to Decrease O2Binding Affinity when exercising? Many students find this confusing, but this actually causes O2 delivery to increase because more O2 leaves the blood in an exercising tissue! • In a healthy lung, all Hb in RBCs gets 100% oxygenated at alveolar exit regardless of how O2-depleted Hb was upon alveolar entry! • Don’t Forget: As CO increases, blood-lung transit time is decreased! • Three Mechanisms to Push oxygen Off Hemoglobin: • 1) Bohr Effect: protons(H+) ↓ O2 affinity • 2) Increased Temperature: ↓ O2 affinity • 3) Biphosphoglycerate and the red blood cell ↓ O2 Affinity • Haldane Effect: O2 removal from Hb increases Hb- O2 affinity! • Carbon Monoxide (CO) binds Hb tighter than O2, so O2 cannot displace the tightly bound CO and O2 can’t get picked up by the hemoglobin as it passed through the lung!
How do we improve oxygen unloading/delivery to a tissue? How do we improve CO2 transport away from a tissue? Shifting the curve Down and to the Right causes O2 to escape the heme and become delivered to the surrounding tissues which can then use it to make ATP
Bohr Effect describes how protons (H+; acidity) affect the properties of hemoglobin and O2/CO2 delivery to a tissue/lung! • 1)H+ increases O2 delivery by pushing O2 off Hb! • 2)H+ leads to acidosis! • 3)H+ can exit body via lung: “Respiratory Compensation” • 4) Carbonic Anhydrase Rxn: One Tissue CA and One Lung CA • Two locations of CA: to Make or Destroy CO2 • Respiratory pH Compensation: “Lung CA provides a quick pH Fix!” • If blood alkaline stop breathing (accumulate CO2 and H+) • If blood acidic hyperventilate and release CO2 and protons. • 5) What happens when you run out of bicarbonate (HCO3-)? • With Hyperventilation? At High Altitude?
CO2 gas solubility in the blood is (like O2) very limited, so we: 1) Reversibly convert CO2 to bicarbonate (HCO3- ) with CA (70%)2) Carry CO2 on deoxygenated Hb molecules in RBCs (23%)3) Let CO2 move freely dissolved in blood (7%)-Tiny Amount! Only a small amount can dissolve as a gas in blood Only a small amount can dissolve as a gas in blood
Hemoglobin in blood that passes through gas-exchange regions of the lung (alveoli/respiratory bronchioles) is RAPIDLY oxygenated to 100% saturation
WHAT HAPPENS WHEN THE PLEAURAL CAVITY VACUUM IS LOST? • Pneumothorax: presence of air in thoracic cavity (puncture). • Atelectasis: collapse of alveoli/lung due to internal tension • 3 Types of Pneumothorax: • 1) Open Pneumo- permits 2-way air flow in/out of thorax, but only one side effected. • 2) Tension Pneumo- Most dangerous: hole in thoracic wall is 1-way valve so air cant leave>>>> • Eventually the intact lung can’t inflate/deflate because otherside is over-filled with air. • 3) Closed Pneumo-Rupture of lung/pleural lining, gas enters and lung collapses: TB, Cough, Emphysema, often self-resolves itself.
Artificial respiration can be done with positive or negative pressure! There are 3 Types of Pneumothorax: Open, Tension and Closed! “Closed”: rupture of the lung and air escapes/enters pleural cavity.
FEV1 Amount of air expired in 1 second with maximal effort: Asthma FCV: Vital Capacity as % of Control: Fibrosis
Gas partial pressures are very important to consider, especially for those who may work with anesthesia in the future! Total P=760 mmHg: N2=597, O2=159, H2O=3.7 and CO2=0.3mmHg. Alveolar Air Partial Pressure: N2=569, O2=104, H2O=47 CO2=40mmHg. Test Question for Test#2: Fill in the blanks with the correct partial pressures.
What terms describe a person’s breathing pattern? • Normal Respiration: 12 bpm @ 500 ml TV • Eupnea: quiet normal TV • Dyspnea: Sense of shortness and gasping • Apnea: breathing temporarily stops • Respiratory Arrest: Full stop • Hypernea: Increased rate • Hypoventilation: Breath too slow • Hyperventilation: Breath to fast • Herring Bauer Reflex: VIP-Protective stretch reflex to stop excessive inspiration • Cheyne-Stokes Breathing: very deep and using O2 as the stimulus • Breaking Point: when you cant breath hold any more
What volumes of air pass through the lung per minute? What is the importance of these minute respiratory volumes (V=ml gas/min)? • Oxygen consumed per minute is called: • VO2=ml O2/minute-kg Values: 250 ml O2/min at rest for whole body VO2 max is 4000 ml O2/min for the whole body or more • Carbon dioxide delivered to lung per minute is called: • VCO2 =ml CO2/minute • Values: 200 ml/min at rest for whole body • VCO2 max is about 8000 ml/min • What are the limits to VO2 consumption (delivery)? • Cardiac Output L/R-side- Hemoglobin- • Fluid-Gas Solubility- • Blood Volume- • Packed Cell Volume/Hematocrit- • Local environment (CO2, H+, temperature)-