Download
1 / 51
780 likes | 2.26k Vues
Osteoarthritis and Osteoporosis. Rochelle M. Nolte, MD CDR USPHS. Objectives. Participants will be able to: Discuss the epidemiology of osteoarthritis and osteoporosis in the geriatric population List 3 risk factors for osteoarthritis and osteoporosis in the geriatric population

E N D
Osteoarthritis and Osteoporosis Rochelle M. Nolte, MD CDR USPHS
Objectives • Participants will be able to: • Discuss the epidemiology of osteoarthritis and osteoporosis in the geriatric population • List 3 risk factors for osteoarthritis and osteoporosis in the geriatric population • Describe the management of osteoarthritis and osteoporosis in the geriatric population
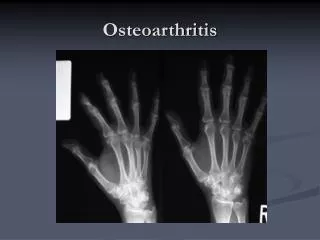
What is Osteoarthritis? According to the American College of Rheumatology: a heterogeneous group of conditions that leads to joint symptoms which are associated with defective integrity of the articular cartilage in addition to related changes in the underlying bone at the joint margins.
Etiology of Osteoarthritis • Growth of cartilage and bone at the joint margins leads to osteophytes which can restrict movement • Chronic synovitis and thickening of the joint capsule further restrict movement • Periarticular muscle wasting is common and plays a major role in sx and disability
Symptoms of osteoarthritis • PAIN (Articular cartilage is aneural) • OA pain is not from the cartilage • Stretching of nerve ending in periosteum covering osteophytes • Microfractures in subchondral bone • Stretching of joint capsule • Synovitis • Ligament stretching or muscle pain • STIFFNESS (esp. after inactivity)
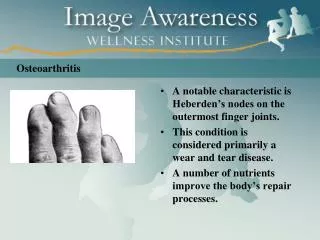
Epidemiology of OA • OA of the knee is the leading cause of chronic disability in the elderly in developed countries • Estimated $60 billion economic impact in US • Decreased quality of life for > 20 million Americans • In patients over the age of 55: • Hip OA is more common in men • IP and 1st MCP OA is more common in women • Knee OA (with sx) is more common in women
Epidemiology of OA • In patients under the age of 55: • Joint distribution of OA is equal between men and women • Due to genetics or joint usage????? • Mother and sister of a woman with DIP OA are 2 & 3 X more likely to have the same • Racial differences in prevalence and pattern of joint involvement also point to genetic basis
Epidemiology of OA • Age is the most powerful risk factor for OA • Women < 45 years of age: 2% with OA • Women 45-64: 30% with OA • Women >65: 68% with OA
Epidemiology of OA • Does exercise cause osteoarthritis?
Epidemiology of OA • There is no convincing data to support an association between nonspecific nonprofessional athletic activities and osteoarthritis • (excluding major trauma) • Neither long-distance running nor jogging has been shown to cause osteoarthritis
Epidemiology of OA • Exercise does not cause osteoarthritis
Epidemiology of OA • OBESITY causes osteoarthritis
Epidemiology of OA • Obesity is a risk factor for knee (and hand) osteoarthritis • In the highest quintile of BMI • Relative risk of developing OA in the next 36 years was 1.5 for men and 2.1 for women • For SEVERE OA, the RR rose to 1.9 for men and 3.2 for women • Weight loss of 5kg was associated with a 50% reduction in the odds of developing OA
Epidemiology of OA • Disability in subjects with knee OA • More strongly associated with QUADRICEPS WEAKNESS • than with joint pain or radiographic severity • Demographics associated with increased likelihood of being symptomatic: women, unemployed, divorced, poor social support
Major joint trauma Repetitive stress Vocational Recreational Obesity Muscle weakness Joint laxity Proprioception loss Risk factors for OA • Age • Sex • Race • Genetic factors • Congenital defects • Malalignment • Prior inflammatory disease • Metabolic disorders
Risk factors for OA • Systemic • Age • Gender • Ethnicity • Genetics • Hormonal status • Bone density • Metabolic/nutritional status
Risk factors for OA • Local • Obesity • Major trauma • Joint deformity/laxity • Physical disability • Muscle weakness • Loss of proprioception • Occupational/sports stress
Prevention of OA • Physical activity is the best way to ensure the maintenance of functional capacity • Physical activity also aids in the prevention of obesity
Prevention of Osteoarthritis • Weight reduction (IA) • Recreational exercise/sports (IA) • Maintain physical fitness (B) • Avoid obesity (B) • Participate in adequate physical exercise (B)
Prevention of OA • Current studies • Isokinetic exercise for improving knee flexor and extensor muscles in healthy adults to assess safety and effectiveness • Will also assess in adults with neurological, orthopedic, and rheumatological conditions • Currently < 1% of money spent on Osteoarthritis is spent on research
Management/Treatment of OA • Goals • Educate patient about disease and management • Improve function • Control pain • Alter disease process and its consequences • (we just don’t know that much about biomarkers and disease-modifying drugs just yet……)
Management/Treatment of OA • No known cure for OA • HOWEVER • Impaired muscle function • Reduced fitness • Affect pain and dysfunction • Are amenable to therapeutic exercise
Pharmacologic Acetaminophen NSAIDS Cox-2 specific inhibitors With PPI or misoprostol Nonacetylated salicylate Tramadol Opioids Topical Capsaicin Methylsalicylate NSAIDS Intra-articular Corticosteroids Hyaluronan Management/Treatment of OA
Non-pharmacologic Patient education Self-management programs Weight loss PT/OT ROM exercises Muscle strengthening Non-pharmacologic Assistive devices Patellar taping Appropriate footwear Lateral-wedged insoles Bracing Joint protection and energy conservation Management/Treatment of OA
Osteoarthritis Summary • Non-pharmacologic therapy is important for the prevention and treatment of OA • The best-studied and most effective non-pharmacologic therapy is EXERCISE • Exercise helps control weight, increase strength, improve and maintain function and decrease pain
Osteoporosis • Skeletal disorder characterized by diminished bone strength predisposing a person to an increased risk of fracture
Osteoporosis • Bone is dependent on nutritional, hormonal, and mechanical influences • Normal remodeling has equal rates of formation and resorption
Demographics of Osteoporosis • In 2004 • 10 million American women with osteoporosis (OP) • 34 million American women with osteopenia • Women >50 • 20% with OP • 52% low BMD
Demographics of Osteoporosis • 1.5 million OP related fx per year in US • 500,000 hospitalizations • 800,000 Emergency Room visits • 2.6 million physician visits • 180,000 nursing home (NH) placements • $18 billion in direct health care costs
Hip Fractures • 300,000 hip fractures per year in US • Over ½ occur in >80 year old patients • ½ of hip fracture patients go to NH • ½ d/c’d to NH become long-term resident • One year mortality is 20%-24% • 60% never return to baseline function • > ½ women >75 prefer death to hip fx
Low BMD Age Previous fx Fall in past year Low body weight Maternal history of hip fracture H/O amenorrhea Asian or white Cigarette smoking Excessive EtOH use Low Ca2+ intake Vitamin D deficiency Long-term immobilization Osteoporosis/Hip fx Risk Factors
Hypogonadal states Glucocorticoid use Excess thyroid Hyperparathyroidism Hypercalciuria Malabsorption states Renal failure Rheumatoid arthritis COPD Alcoholism Chronic Liver Disease Organ transplant Malnutrition Eating disorders Type I DM Medications Secondary Osteoporosis
Osteoporosis Prevention • Adequate caloric intake • Exercise • Weight-bearing • Swimming • Intermittent dynamic loading • Avoid tobacco • Avoid/decrease alcohol intake
Osteoporosis Prevention • 92% of total bone mass by age 18 • 99% by age 26 • Bone mass not obtained during this time cannot be made up later
Osteoporosis prevention • Different sites mature at different ages • Peak bone mass complete by age 16 in the femoral neck • Later in lumbar spine and distal radius
Osteoporosis Prevention • Adequate caloric intake • Calcium 500mg mg TID • Vitamin D 800 IU qd • May consider OCP’s if above are met • Goal is to restore reproductive and metabolic hormones by increasing energy availability
Osteoporosis Management • Goals of osteoporosis management • Prevention of fracture • Stabilization or increase of bone mass • Relief of sx of fx and skeletal deformity • Maximization of physical function
Osteoporosis Management • Non-pharmacologic management • Same as for osteoporosis prevention • Nutritional • Calcium 500mg TID • Vitamin D 80 IU qd
Pharmacologic Management • Estrogen Therapy • Not approved for treatment (only prevention) • Bisphosphonates • Approved for prevention and treatment • Therapy of first choice • Selective Estrogen Receptor Modulators • Approved for prevention and treatment • Raloxifene
Pharmacologic Management • Calcitonin • Approved for treatment of osteoporosis in women who have been postmenopausal for >5 years • Bisphosphonates seem to be more efficacious • Anabolic Therapy (teriparatide) • Daily SubQ injection • Approved for treatment in high risk patients
Physicians’ challenges • Identify potential osteoporosis risk factors • Educate patients • Initiate interventions proactively • PREVENTION AND DIAGNOSIS OF OSTEOPOROSIS IS FAR FROM WIDESPREAD • Despite Surgeon Generals report in 2004
Missed opportunities • Vertebral fractures noted incidentally • Should be reported and prompt further eval • Patients with history of fragility fractures • Should be evaluated and treated for OP • Women over age 65 or with risk factors • Should be screened with DEXA • Women should be educated on OP
Osteoporosis Summary • Much of what can be done to prevent osteoporosis and osteoporosis-related fractures is not being done • Prevention of osteoporosis begins in childhood • Treatment to prevent osteoporosis-related fractures should be targeted to high risk patients
Summary • Osteoarthritis and osteoporosis are important public health issues in a rapidly enlarging geriatric population • Prevention of both can be promoted through a physically active lifestyle and a healthy diet beginning at a young age