Diabetic Nephropathy
Diabetic Nephropathy. Diabetic Nephropathy. Over 40% of new cases of end-stage renal disease (ESRD) are attributed to diabetes. In 2001, 41,312 people with diabetes began treatment for end-stage renal disease.


Diabetic Nephropathy
E N D
Presentation Transcript
Diabetic Nephropathy • Over 40% of new cases of end-stage renal disease (ESRD) are attributed to diabetes. • In 2001, 41,312 people with diabetes began treatment for end-stage renal disease. • In 2001, it cost $22.8 billion in public and private funds to treat patients with kidney failure. • Minorities experience higher than average rates of nephropathy and kidney disease
Five Stages of Kidney Disease Stage 1: Hyperfiltration, or an increase in glomerular filtration rate (GFR) occurs. Kidneys increase in size. Stage 2: Glomeruli begin to show damage and microalbuminurea occurs. Stage 3: Albumin excretion rate (AER) exceeds 200 micrograms/minute, and blood levels of creatinine and urea-nitrogen rise. Blood pressure may rise during this stage.
Five Stages of Kidney Disease (con’t.) Stage 4: GFR decreases to less than 75 ml/min, large amounts of protein pass into the urine, and high blood pressure almost always occurs. Levels of creatinine and urea-nitrogen in the blood rise further. Stage 5: Kidney failure, or end stage renal disease (ESRD). GFR is less than 10 ml/min. The average length of time to progress from Stage 1 to Stage 4 kidney disease is 17 years for a person with type 1 diabetes. The average length of time to progress to Stage 5, kidney failure, is 23 years.
Screening for Diabetic Nephropathy 1American Diabetes Association:Nephropathy in Diabetes(Position Statement). Diabetes Care 27 (Suppl.1): S79-S83, 2004
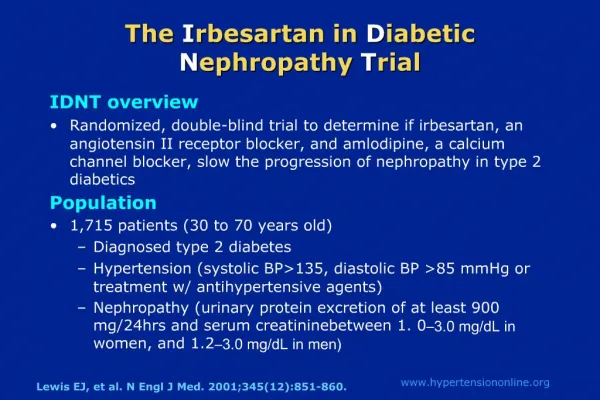
Treatment of Diabetic Nephropathy • Hypertension Control -Goal: lower blood pressure to <130/80 mmHg • Antihypertensive agents • Angiotensin-converting enzyme (ACE) inhibitors • captopril, enalapril, lisinopril, benazepril, fosinopril, ramipril, quinapril, perindopril, trandolapril, moexipril • Angiotensin receptor blocker (ARB) therapy • candesartan cilexetil, irbesartan, losartan potassium, telmisartan, valsartan, esprosartan • Beta-blockers
Treatment of Diabetic Nephropathy (cont.) • Glycemic Control • Preprandial plasma glucose 90-130 mg/dl • A1C <7.0% • Peak postprandial plasma glucose <180 mg/dl • Self-monitoring of blood glucose (SMBG) • Medical Nutrition Therapy • Restrict dietary protein to RDA of 0.8 g/kg body weight per day
Treatment of End-Stage Renal Disease (ESRD) There are three primary treatment options for individuals who experience ESRD: 1. Hemodialysis 2. Peritoneal Dialysis 3. Kidney Transplantation
Hemodialysis • Procedure • A fistula or graft is created to access the bloodstream • Wastes, excess water, and salt are removed from blood using a dialyzer • Hemodialysis required approx. 3 times per week, each treatment lasting 3-5 hrs • Can be performed at a medical facility or at home with appropriate patient training
Hemodialysis (cont.) • Hemodialysis Diet • Monitor protein intake • Limit potassium intake • Limit fluid intake • Avoid salt • Limit phosphorus intake • Complications • Infection at access site • Clotting, poor blood flow • Hypotension
Peritoneal Dialysis • Procedure • Dialysis solution is transported into the abdomen through a permanent catheter where it draws wastes and excess water from peritoneal blood vessels. The solution is then drained from the abdomen. • Three Types of Peritoneal Dialysis • Continuous Ambulatory Peritoneal Dialysis (CAPD) • Continuous Cycler-Assisted Peritoneal Dialysis (CCPD) • Combination CAPD and CCPD
Peritoneal Dialysis (cont.) • Peritoneal Dialysis Diet • Limit salt and fluid intake • Consume more protein • Some potassium restrictions • Reduce caloric intake • Complications • Peritonitis
Kidney Transplant • Procedure • A cadaveric kidney or kidney from a related or non-related living donor is surgically placed into the lower abdomen. • Three factors must be taken into consideration to determine kidney/recipient match: • Blood type • Human leukocyte antigens (HLAs) • Cross-matching antigens
Kidney Transplant (cont.) • Kidney Transplant Diet • Reduce caloric intake • Reduce salt intake • Complications/Risk Factors • Rejection • Immunosuppressant side effects • Benefits • No need for dialysis • fewer dietary restrictions • higher chance of living longer
How Can You Prevent Diabetic Kidney Disease? • Maintain blood pressure <130/80 mm/Hg • Maintain preprandial plasma glucose 90-130 mg/dl • Maintain postprandial plasma glucose <180 mg/dl • Maintain A1C <7.0%
References American Diabetes Association:Nephropathy in Diabetes(Position Statement). Diabetes Care 27 (Suppl.1): S79-S83, 2004 National Kidney and Urologic Diseases Information Clearinghouse. Kidney Disease of Diabetes. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health (NIH), DHHS; 2003. United States Renal Data System. USRDS 2003 Annual Data Report. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health (NIH), DHHS; 2003. DeFronzo RA: Diabetic nephropathy: etiologic and therapeutic considerations. Diabetes Reviews 3:510-547, 1995 National Kidney and Urologic Diseases Information Clearinghouse. Kidney Failure: Choosing a Treatment That’s Right For You. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health (NIH), DHHS; 2003.