Download

1 / 20
601 likes | 4.37k Vues
Congenital Mitral Valve Disease. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery. Congenital Abnormalities of Mitral Valve. Incidence

E N D
Congenital Mitral Valve Disease Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
Congenital Abnormalities of Mitral Valve • Incidence • * 0.2-0.4% of all CHD • * MS : 0.6% in autopsy • MR : 0.5% in autopsy • * Associated lesions : ASD, VSD, PS, COA, LVOTO • Mitral valve malformations may constitute an integral part of • complex lesions such as hypoplastic left heart syndrome, • Shone’s complex, atrioventricular canal, double inlet ventricle. • Pathophysiology • MS (75-80% have associated lesions) • MR • MSR
Pathophysiology of Congenital Mitral Valve Disease • Malformation of the mitral valve apparatus results in mitral stenosis, insufficiency, or both. • Significant flow obstruction or regurgitation of the mitral valve results in elevated pulmonary venous pressure and pulmonary congestion. • Left untreated, pulmonary vascular occlusive changes and pulmonary hypertension lead to right ventricular hypertrophy and right heart failure.
Clinical Features of Congenital Mitral Valve Disease • Symptoms Fatigue, DOE, recurrent pulmonary infection, tachypnea, growth retardation, central cyanosis. Severely affected infants have CHF with gross pulmonary edema • Signs Systolic & diastolic murmur, redistribution of pulmonary vascularity, cardiac enlargement, LA enlargement, increased MPA, LV enlargement in MR
Patterns of Congenital MV Diseases • Mitral Stenosis 1) Associated lesions • 25% isolated • 30% VSD • 40% LVOT obstruction( 2% of COA has congenital MS) • others : TOF, VSD+PS, PS 2) Symptom & signs • usually severe & if untreated, death during 1st 4~5 years of life • Mitral Insufficiency • Often only moderate in severity in early life, and 1/2 patients • come to operation until older than about 5 years of age.
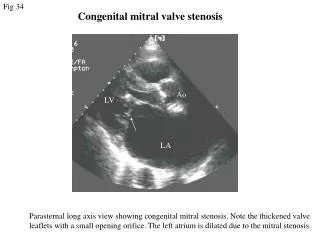
Types of Congenital Mitral Stenosis • Supravalvular • * Fibrous ring • * Shone’s syndrome • Valvular • * Fusion of commissure & papillary muscle • * Double orifice • * Excessive valve tissue • * Annular hypoplasia( usually associated with HLHS) • Subvalvular • * Single papillary muscle (Parachute valve) • * Abnormally large or numerous papillary muscle (Hammock valve) • * Absent papillary muscle # Abnormalities associated with LVOTO • * Abnormal attachment of the subvalvular apparatus to the septum. • * Systolic anterior movement( usually with hypertrophic cardiomyopathy)
Congenital Mitral StenosisFunctional Classification (Carpentier) 1. Normal papillary muscle 1) Commissural & papillary fusion 2) Excessive leaflet tissue 3) Valvar ring 4) Annular hypoplasia 2. Abnormal papillary muscle 1) Parachute mitral valve 2) Hammock mitral valve
Parachute-like Asymmetric Mitral Valve • Unequal distribution of chords • One normal and one elongated papillary muscle • Elongated papillary muscle is displaced toward • the MV annulus. • The anterolateral papillary muscle is usually abnormal. • Clinical implications are mitral stenosis and other malformations are present.
Congenital Mitral Regurgitation • Annulus • 1) Dilation • * secondary due to ventricular dilation ( rare in primary causes) • (endocardial fibroelastosis, infarction, ischemia, ASD) • Leaflets • 1) Cleft • 2) Leaflet defect • * hole due to localized agenesis (posterior) • 3) Mitral valve prolapse • * rupture or elongated chordae tendinea • 4) Congenital perforation or displacement • * Ebstein’s anomaly of MV • 5) Duplication of orifice • Subvalvular apparatus • 1) Bridge of fibrous tissue ( anomalous arcade) with shortened or absent chordae • 2) Shortened chordae tendineae • 3) Abnormal papillary muscle
Congenital Mitral RegurgitationFunctional classification (Carpentier) 1. Normal motion of the leaflet (type I) 1) Deformation & dilatation 2) Clefts 3) Partial agenesis 2. Prolapse of leaflet (type II) 1) Absence of tendinous cords 2) Elongation of tendinous cords 3) Elongation of papillary m. 3. Restricted motion of leaflet (type III) 1) Normal papillary m. commissural fusion / shortness of cords 2) Abnormal papillary m. parachute / Hammock / hypoplasia of papillary m. / Ebstein malformation / double orifice
LV Dysfunction in Mitral Regurgitation • 1. Indicators • 1) NYHA status • 2) Ejection fraction • 3) LV end-diastolic & end-systolic dimension • 4) Rate of rise of LV pressure • 5) Left atrial size • 6) Pulmonary artery pressure • 2. Misleading • It is possible to have LV dysfunction in the presence • of normal LV dimension & minimal symptoms due to • afterload reduction of the regurgitant mitral valve.
Pulmonary Hypertension in MVD • 1. Increased LAP transmitted on a retrograde • basis into the arterial circulation • 2. Vascular remodeling of pulmonary vasculature • in response to chronic obstruction to pulmonary • venous drainage(fixed component) • 3. Pulmonary arterial vasoconstriction • (reactive component)
Indications for Mitral Valve Operation • Severe symptoms & signs of important pulmonary venous hypertension are indications of mitral valve anomalies • Infancy • 1) Mild to moderate symptoms with certainty without valve • replacement : supravalvular ring, commissure fusion • 2) Other circumstances • reserved only for infants with intractable heart failure • Childhood • 1) Considerations for operation are similar • * CHF • * pulmonary hypertension secondary to MVD • 2) MVR should be withheld whenever possible
Operative Procedures for Mitral Valve • 1. Mitral regurgitation • 1) Eccentric annuloplasty • 2) Ring annuloplasty • 3) Leaflet plication & chordal shortening • 4) Suture of cleft • 5) Valve replacement • 2. Mitral obstruction • 1) Resection of supravalvular ring • 2) Open commissurotomy & splitting • 3) Correction of parachute deformity : splitting & fenestration • 4) Valve replacement
Mitral Valve Repair for Multiple Leaflets • Remodeling the annulus with Ring(1) after annular plication with resected posterior median leaflet(2)
Anatomy of Mitral Annulus • C-shaped portion touches the underlying LV • wall, the remaining 25-30% of annulus is • intracavitary. • Muscular representation is the basis for • geometric relationship, being more elliptic • in systole and circular in diastole. • * To be a support for the leaflet attachment • * To insulate electrically the atrium from ventricle
Aims for Mitral Valve Annuloplasty • Reduce annular dilation & mitral valve area • Increase the leaflet coaptation • Reinforce the annulus sutures when part of • the valve has been resected • Prevent future dilation of annulus • ( Stabilization of the posterior annulus )
Complications of Mitral Annuloplasty Ring 1. Postoperative valvular incompetence most common ; mild in 15% by Echo 2. LVOT obstruction : 3% 3. Suture line dehiscence : 2% 4. Dehiscence of prosthetic ring, fracture, hemolysis : 1% 5. Aortic regurgitation : infrequent
Postoperative Course & Results • Mortality • * Usually higher than adult ( LCO, pulmonary hypertension) • Complication • * Low cardiac output * Neurologic complication • * Bleeding and infection * Arrhythmia • * Pulmonary insufficiency • Risk factors • * Young age • * Preoperative functional status • * Associated cardiac anomaly • Long-term result • * Most survivors improve functionally. • * Better for mitral valve repair than replacement • * Residual stenosis or regurgitation is present in most & can progress.